

Knowledge translation and process improvement interventions increased pain assessment documentation in a large quaternary paediatric post-anaesthesia care unit
- PMID: 30167475
- PMCID: PMC6112407
- DOI: 10.1136/bmjoq-2018-000319
Knowledge translation and process improvement interventions increased pain assessment documentation in a large quaternary paediatric post-anaesthesia care unit
Abstract
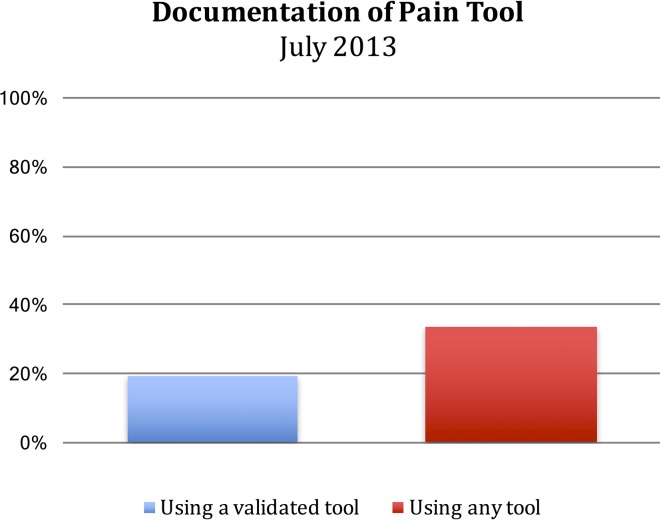
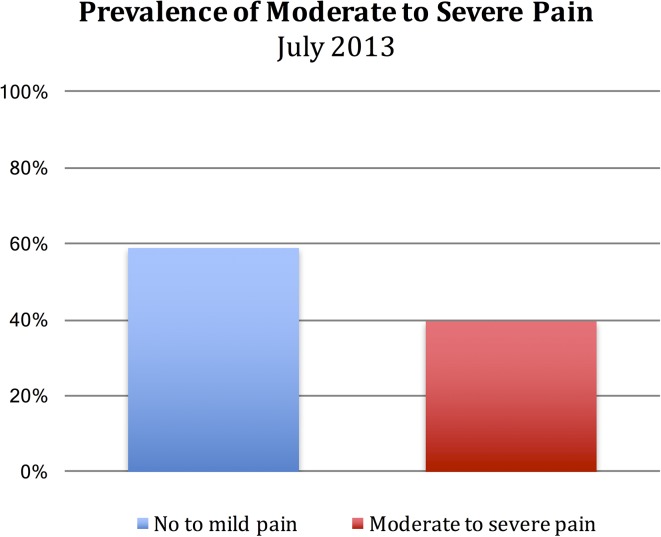
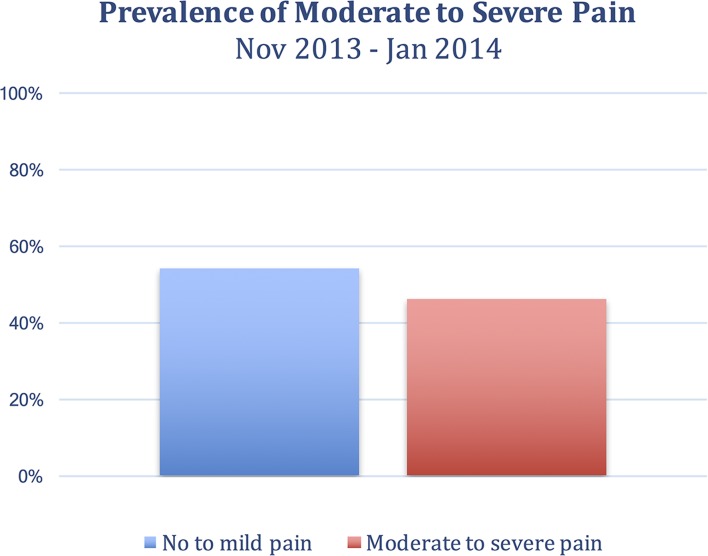
Background: Due to inadequate pain assessment documentation in our paediatric post-anaesthetic care unit (PACU), we were unable to monitor pain intensity, and target factors contributing to moderate and severe postoperative pain in children. The purpose of this study was to improve pain assessment documentation in PACU through a process improvement intervention and knowledge translation (KT) strategy. The study was set in a PACU within a large university affiliated paediatric hospital. Participants included PACU and Acute Pain Service nursing staff, administrative staff and anaesthesiologists.
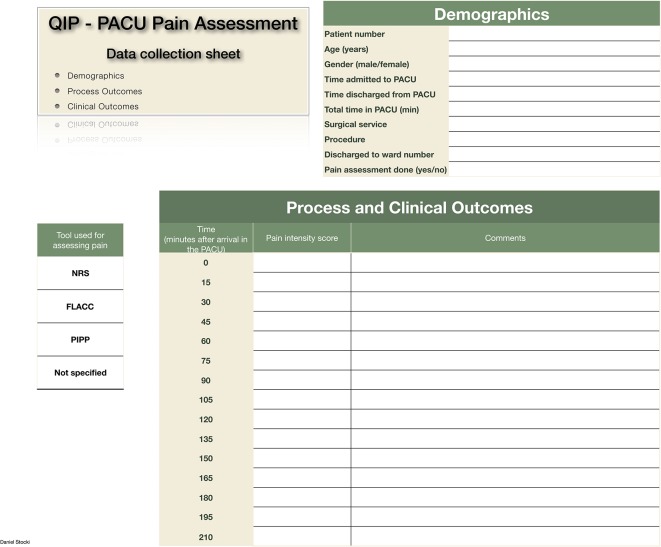
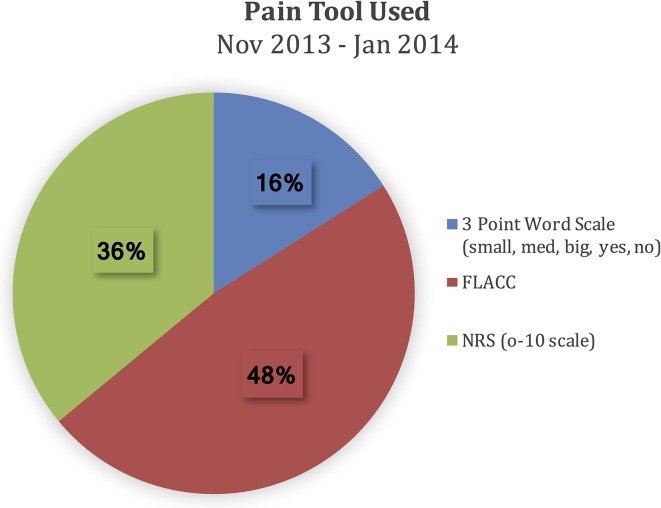
Methods: The Plan-Do-Study-Act method of quality improvement was used. Benchmark data were obtained by chart review of 99 patient medical records prior to interventions. Data included pain assessment documentation (pain intensity score, use of validated pain intensity measure) during PACU stay. Repeat chart audit took place at 4, 5 and 6 months after the intervention.
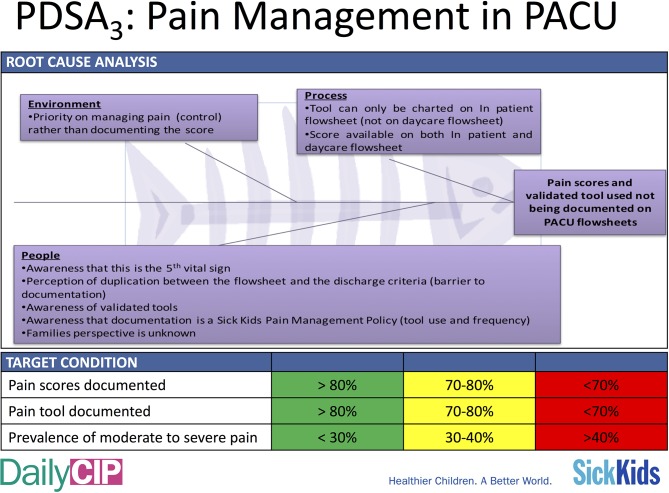
Intervention: Key informant interviews were conducted to identify barriers to pain assessment documentation. A process improvement was implemented whereby the PACU flowsheets were modified to facilitate pain assessment documentation. KT strategy was implemented to increase awareness of pain assessment documentation and to provide the knowledge, skill and judgement to support this practice. The KT strategy was directed at PACU nursing staff and comprised education outreach (educational meetings for PACU nurses, discussions at daily huddles), reminders (screensavers, bedside posters, email reminders) and feedback of audit results.
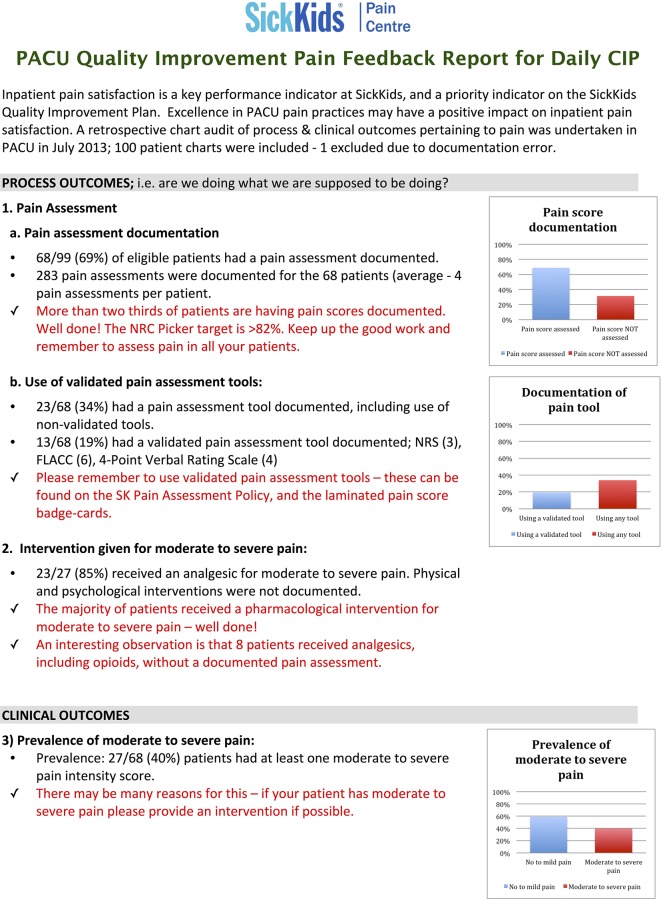
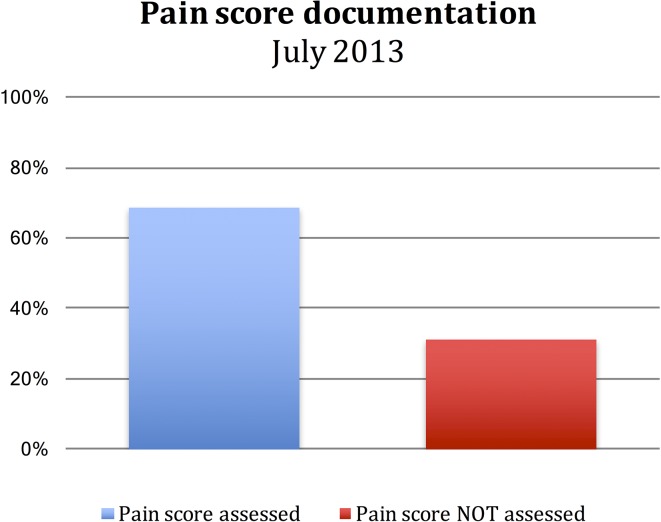
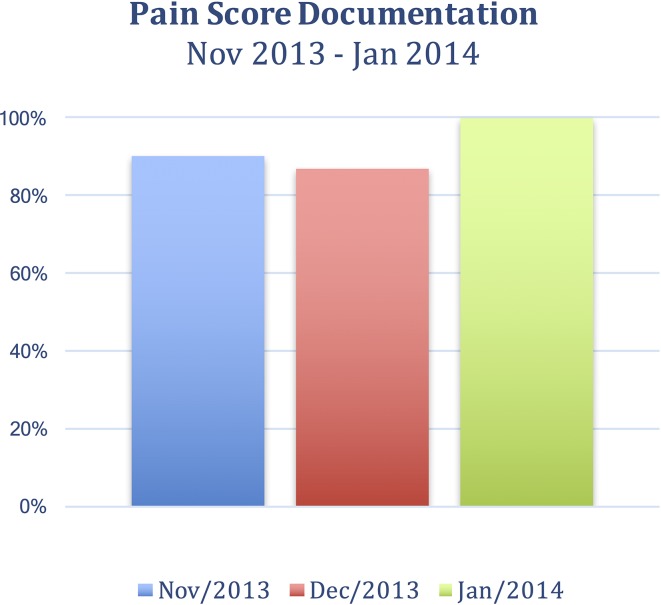
Results: The proportion of charts that included at least one documented pain assessment was 69%. After intervention, pain assessment documentation increased to >90% at 4 and 5 months, respectively, and to 100% after 6 months.
Conclusion: After implementing process improvement and KT interventions, pain assessment documentation improved. Additional work is needed in several key areas, specifically monitoring moderate to severe pain, in order to target factors contributing to significant postoperative pain in children.
Keywords: audit and feedback; paediatrics; pain; pdsa; quality improvement.
Conflict of interest statement
Competing interests: None declared.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources