

One-Year Safety and Clinical Outcomes of a Transcatheter Interatrial Shunt Device for the Treatment of Heart Failure With Preserved Ejection Fraction in the Reduce Elevated Left Atrial Pressure in Patients With Heart Failure (REDUCE LAP-HF I) Trial: A Randomized Clinical Trial
- PMID: 30167646
- PMCID: PMC6233816
- DOI: 10.1001/jamacardio.2018.2936
One-Year Safety and Clinical Outcomes of a Transcatheter Interatrial Shunt Device for the Treatment of Heart Failure With Preserved Ejection Fraction in the Reduce Elevated Left Atrial Pressure in Patients With Heart Failure (REDUCE LAP-HF I) Trial: A Randomized Clinical Trial
Abstract
Importance: In patients with heart failure (HF) and left ventricular ejection fraction (LVEF) equal to or greater than 40%, a transcatheter interatrial shunt device (IASD; Corvia Medical) reduces exercise pulmonary capillary wedge pressure (PCWP) and is safe compared with sham control treatment at 1 month of follow-up. The longer-term safety and patency of the IASD has not yet been demonstrated in the setting of a randomized clinical trial (RCT).
Objective: To evaluate the 1-year safety and clinical outcomes of the IASD compared with a sham control treatment.
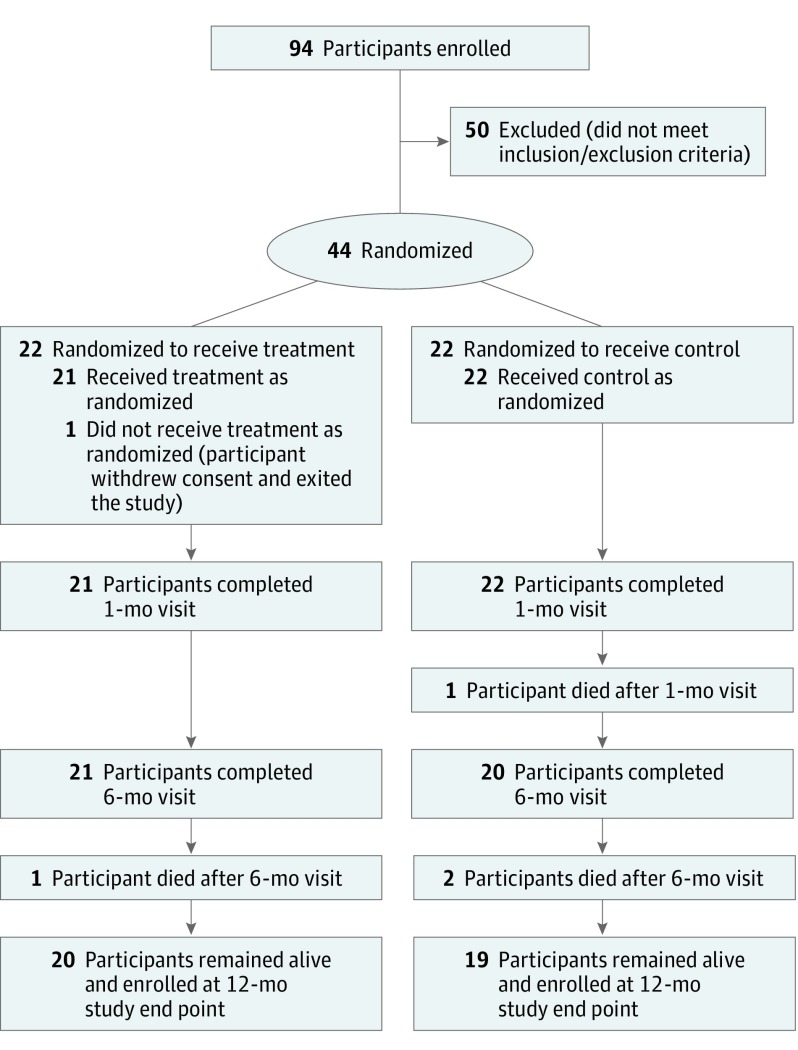
Design, setting, and participants: This phase 2, double-blind, 1-to-1 sham-controlled multicenter RCT of IASD implantation vs a sham procedure (femoral venous access and imaging of the interatrial septum without IASD) was conducted in 22 centers in the United States, Europe, and Australia on patients with New York Heart Association (NYHA) class III or ambulatory class IV HF, LVEF equal to or greater than 40%, exercise PCWP equal to or greater than 25 mm Hg, and PCWP-right atrial pressure gradient equal to or greater than 5 mm Hg.
Main outcomes and measures: Safety was assessed by major adverse cardiac, cerebrovascular, or renal events (MACCRE). Exploratory outcomes evaluated at 1 year were hospitalizations for HF, NYHA class, quality of life, a 6-minute walk test, and device patency.
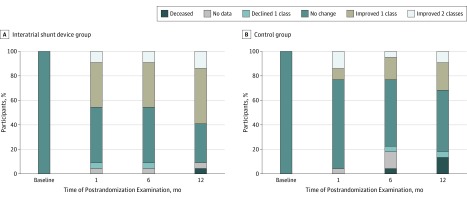
Results: After 1 year, shunts were patent in all IASD-treated patients; MACCRE did not differ significantly in the IASD arm (2 of 21 [9.5%]) vs the control arm (5 of 22 [22.7%]; P = .41), and no strokes occurred. The yearly rate of hospitalizations for HF was 0.22 in the IASD arm and 0.63 in the control arm (P = .06). Median improvement in NYHA class was 1 class in the IASD arm (IQR, -1 to 0) vs 0 in the control arm (IQR, -1 to 0; P = .08). Quality of life and 6-minute walk test distance were similar in both groups. At 6 months, there was an increase in right ventricular size in the IASD arm (mean [SD], 7.9 [8.0] mL/m2) vs the control arm (-1.8 [9.6] mL/m2; P = .002), consistent with left-to-right shunting through the device; no further increase occurred in the IASD arm at 12 months.
Conclusions and relevance: The REDUCE LAP-HF I phase 2, sham-controlled RCT confirms the longer-term patency of the IASD. Through 1 year of follow-up, IASD treatment appears safe, with no significant differences in MACCRE in patients receiving IASD compared with those who received sham control treatment.
Trial registration: ClinicalTrials.gov identifier: NCT02600234.
Conflict of interest statement
Figures

Comment in
-
Evaluating Treatment Effect of Transcatheter Interatrial Shunt Device Using Heart Failure Event Rates-Reply.JAMA Cardiol. 2019 Mar 1;4(3):299-300. doi: 10.1001/jamacardio.2019.0004. JAMA Cardiol. 2019. PMID: 30785592 No abstract available.
-
Evaluating Treatment Effect of Transcatheter Interatrial Shunt Device Using Heart Failure Event Rates.JAMA Cardiol. 2019 Mar 1;4(3):299. doi: 10.1001/jamacardio.2019.0001. JAMA Cardiol. 2019. PMID: 30785598 No abstract available.
References
-
- Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Rev Esp Cardiol (Engl Ed). 2016;69(12):1167. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017;136(6):e137-e161. doi: 10.1161/CIR.0000000000000509 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
