

Advances in Understanding the Pathophysiology of Lacunar Stroke: A Review
- PMID: 30167649
- PMCID: PMC7426021
- DOI: 10.1001/jamaneurol.2018.1073
Advances in Understanding the Pathophysiology of Lacunar Stroke: A Review
Abstract
Importance: Stroke is the second leading cause of death in the world, and nearly one-third of ischemic strokes are lacunar strokes (LSs) or small subcortical infarcts. Although smaller in size, they create large problems, leaving many patients with intellectual and physical disabilities. Because there are limitations in understanding the underlying pathophysiology of LS, the development of novel therapies has been slow.
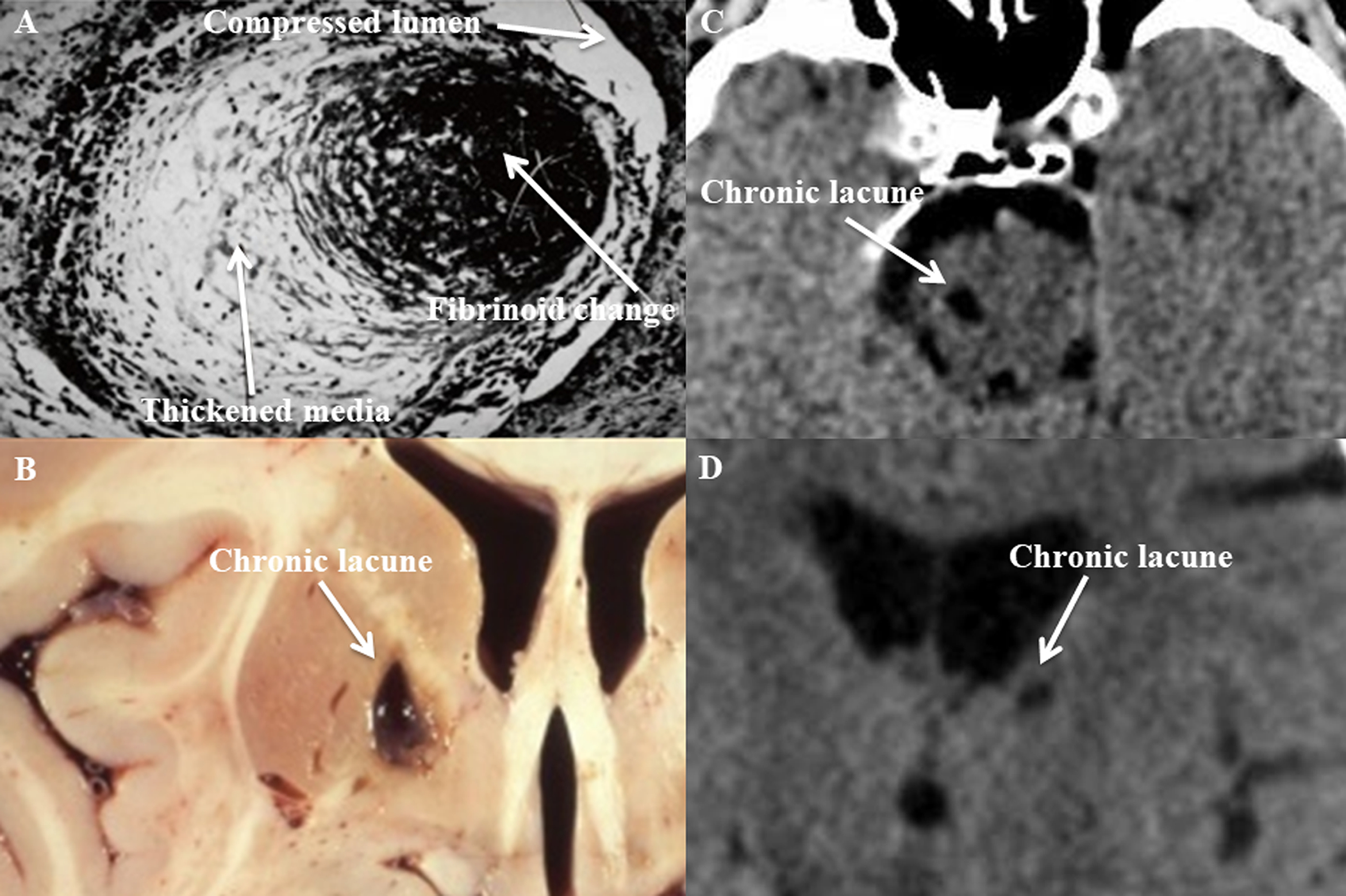
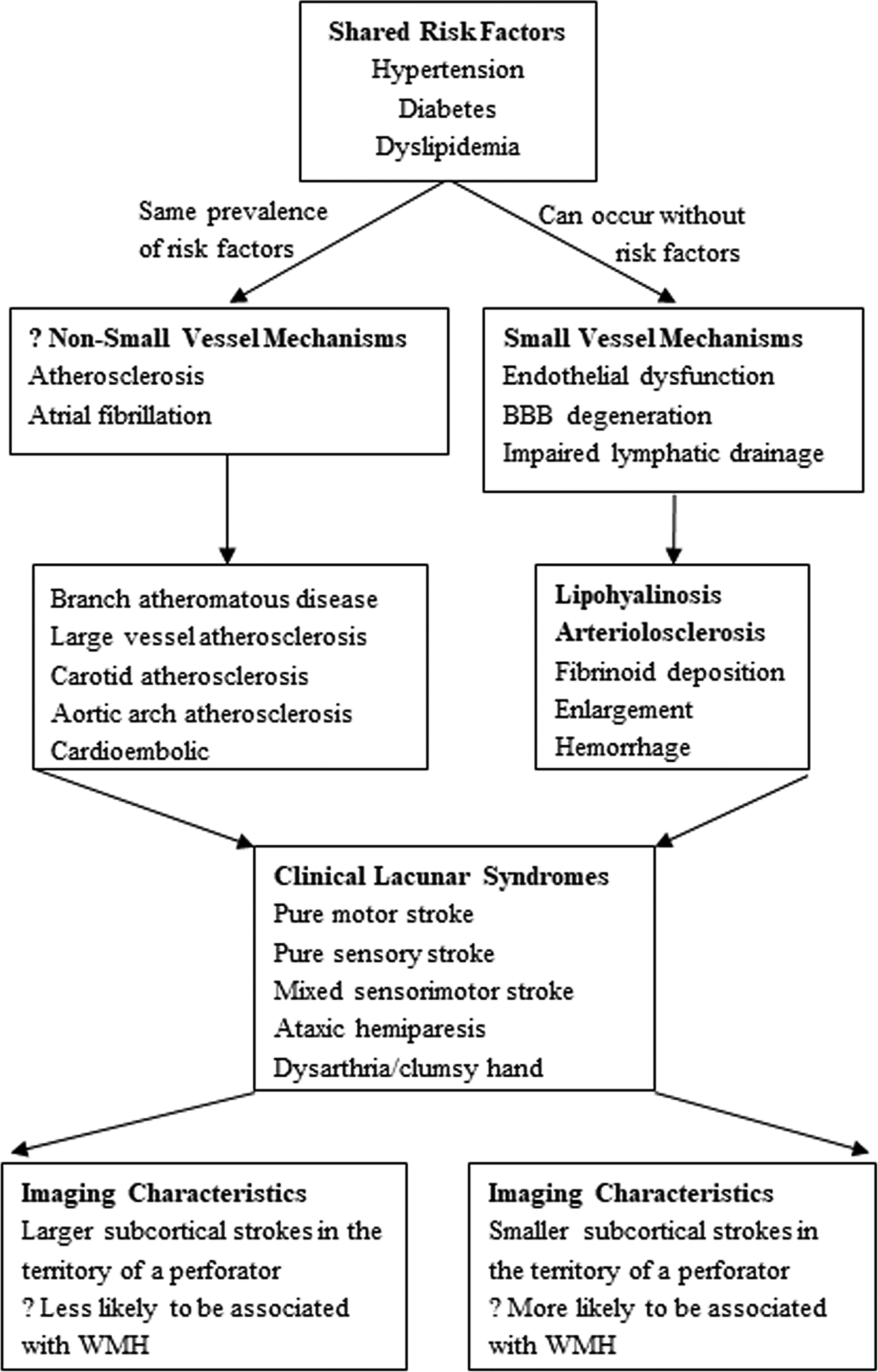
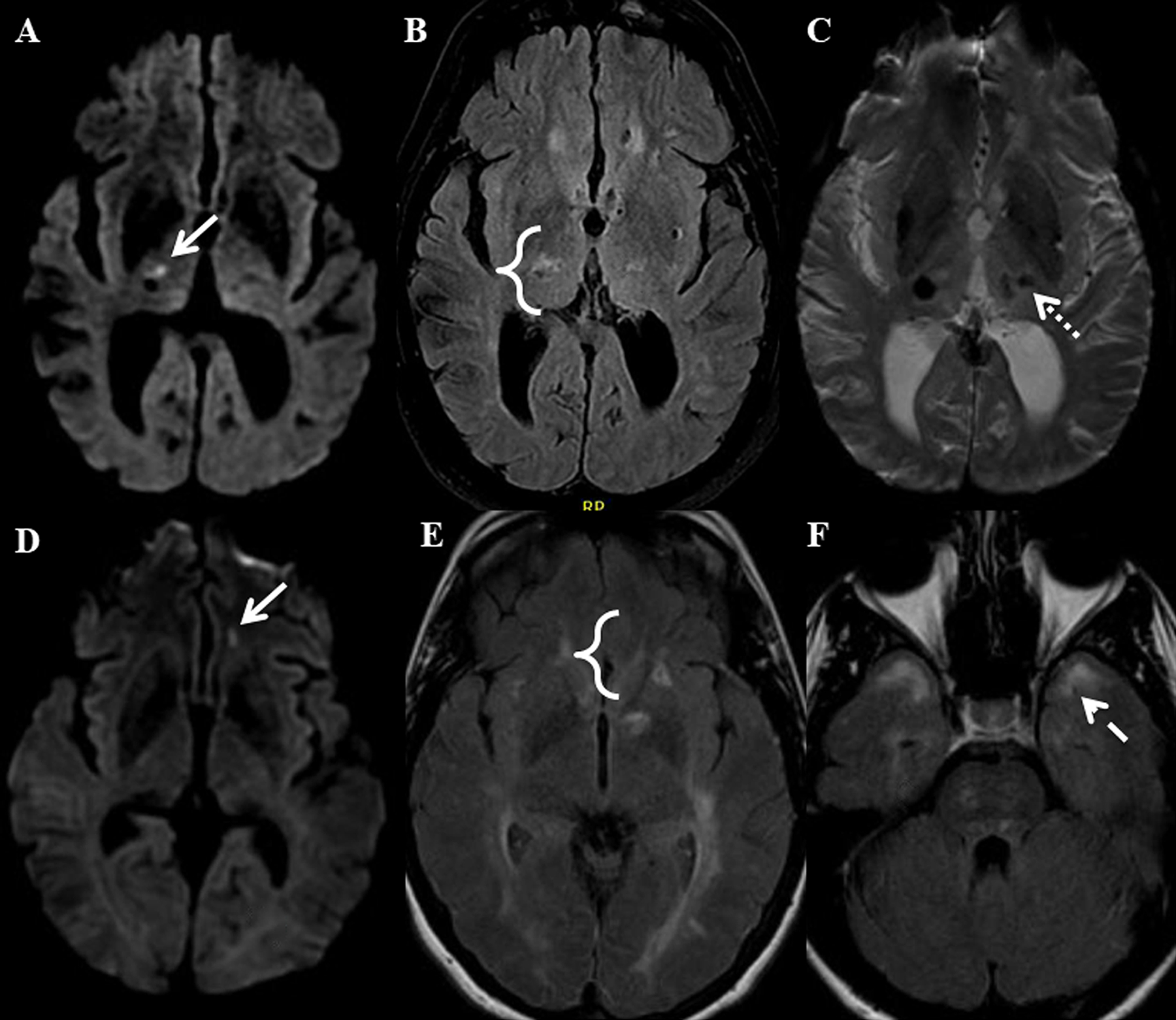
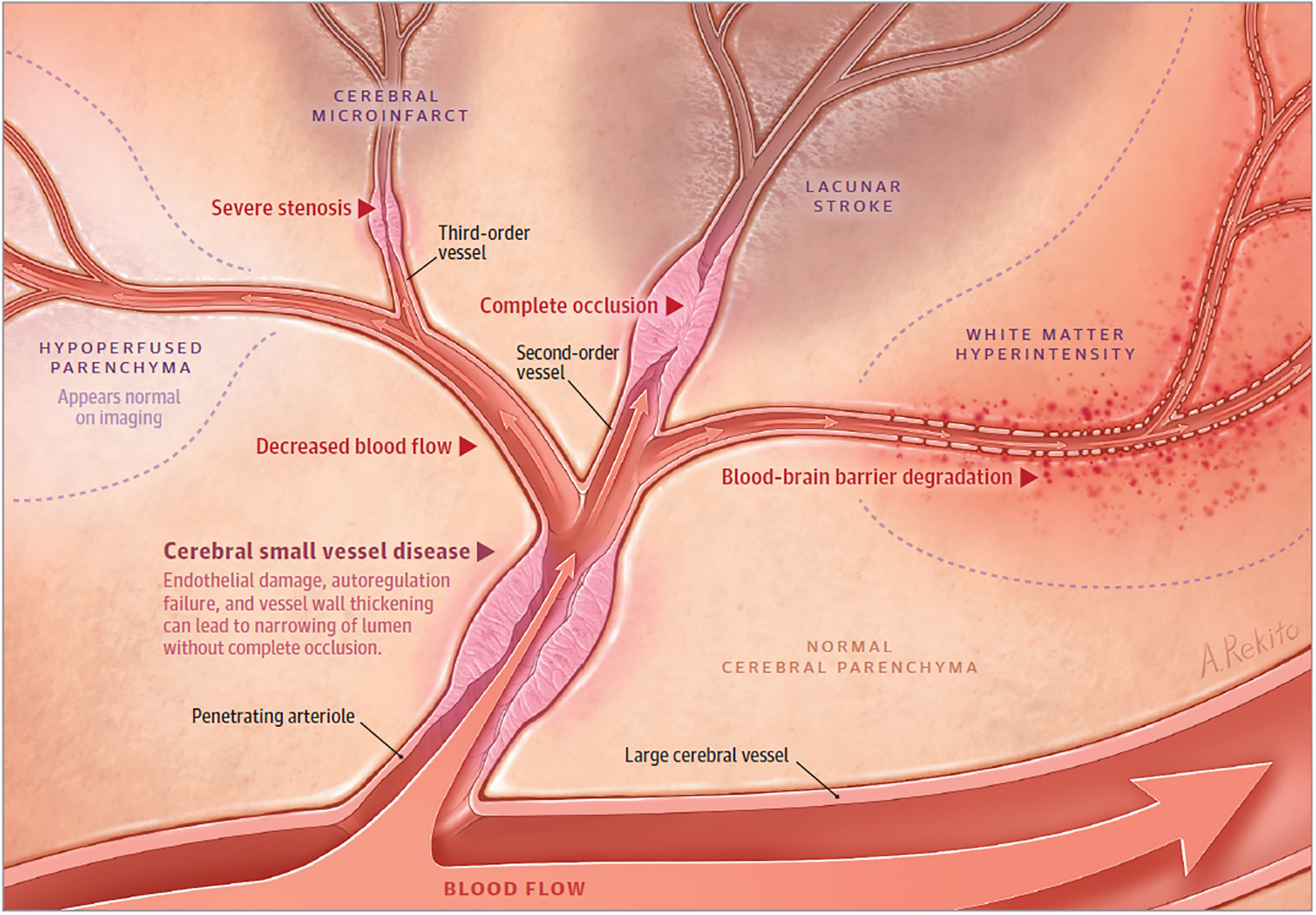
Observations: When the term lacune was described in the 1800s, its underlying pathophysiological basis was obscure. In the 1960s, C. Miller Fisher, MD, performed autopsy studies that showed that vessels supplying lacunes displayed segmental arteriolar disorganization, characterized by vessel enlargement, hemorrhage, and fibrinoid deposition. For these pathologic changes, he coined the term lipohyalinosis. Since that time, few attempts have been made to reconcile this pathologic description with modern mechanisms of cerebral small vessel disease (CSVD). During the past 6 years, progress has been made in understanding the clinical mechanisms, imaging characteristics, and genetic basis of LS.
Conclusions and relevance: Questions persist regarding the order of events related to the initiation and progression of CSVD, how LS is related to other sequelae of CSVD, and whether LS is part of a systemic disease process. The relative roles of aging, oxidative stress, mechanical stress, genetic predisposition, and other vascular risk factors should be further studied, especially in the era of widespread antihypertensive use. Although understanding of endothelial dysfunction has increased, future work on the role of media and adventitial dysfunction should be explored. Recent advances in mapping the brain vasculome may generate new hypotheses. The investigation of new therapeutic targets, aimed at reversing CSVD processes and promoting neural repair after LS, depends upon further understanding these basic mechanisms.
Figures
Comment in
-
The Importance of Blood Pressure Gradients in the Brain: Cerebral Small Vessel Disease.JAMA Neurol. 2019 Mar 1;76(3):370-371. doi: 10.1001/jamaneurol.2018.4627. JAMA Neurol. 2019. PMID: 30715079 No abstract available.
References
-
- Norrving B Long-term prognosis after lacunar infarction. Lancet Neurol. 2003;2(4):238–245. http://www.ncbi.nlm.nih.gov/pubmed/12849212. Accessed August 11, 2017. - PubMed
-
- Fisher CM. The arterial lesions underlying lacunes. Acta Neuropathol. 1968;12(1):1–15. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
