

Effect of Dextroamphetamine on Poststroke Motor Recovery: A Randomized Clinical Trial
- PMID: 30167675
- PMCID: PMC6583201
- DOI: 10.1001/jamaneurol.2018.2338
Effect of Dextroamphetamine on Poststroke Motor Recovery: A Randomized Clinical Trial
Abstract
Importance: Data from animal models show that the administration of dextroamphetamine combined with task-relevant training facilitates recovery after focal brain injury. Results of clinical trials in patients with stroke have been inconsistent.
Objectives: To collect data important for future studies evaluating the effect of dextroamphetamine combined with physiotherapy for improving poststroke motor recovery and to test the efficacy of the approach.
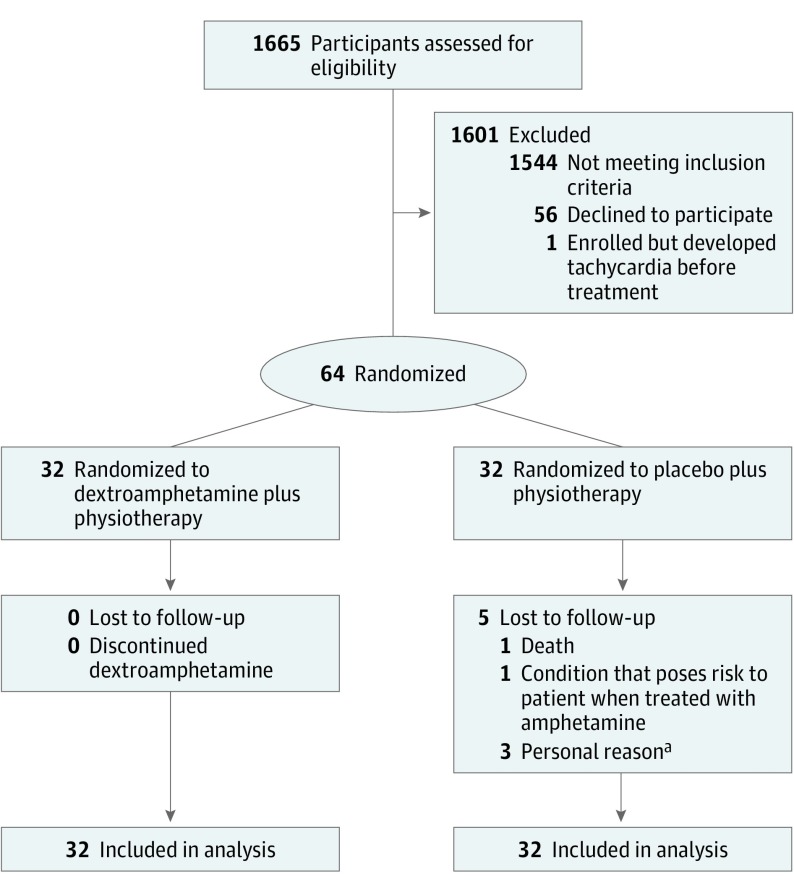
Design, setting, participants: This pilot, double-blind, block-randomized clinical trial included patients with cortical or subcortical ischemic stroke and moderate or severe motor deficits from 5 rehabilitation hospitals or units. Participants were screened and enrolled from March 2001 through March 2003. The primary outcome was assessed 3 months after stroke. Study analysis was completed December 31, 2015. A total of 1665 potential participants were screened and 64 were randomized. Participants had to begin treatment 10 to 30 days after ischemic stroke. Data analysis was based on intention to treat.
Interventions: Participants were allocated to a regimen of 10 mg of dextroamphetamine (n = 32) or placebo (n = 32) combined with a 1-hour physical therapy session beginning 1 hour after drug or placebo administration every 4 days for 6 sessions in addition to standard rehabilitation.
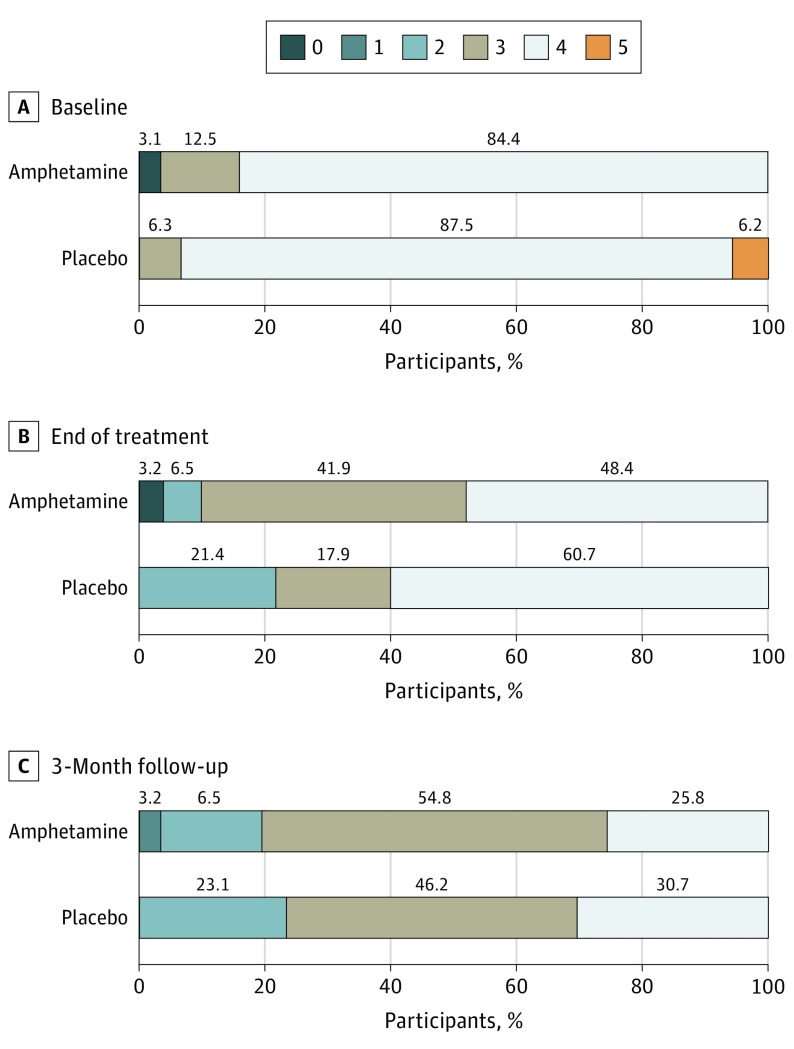
Main outcomes and measures: The primary outcome was the difference between groups in change in Fugl-Meyer motor scores from baseline to 3 months after stroke (intention to treat with dextroamphetamine). Secondary exploratory measures included the National Institutes of Health Stroke Scale, Canadian Neurological Scale, Action Research Arm Test, modified Rankin Scale score, Functional Independence Measure, Ambulation Speed and Distance, Mini-Mental State Examination, Beck Depression Inventory, and Stroke Impact Scale.
Results: Among the 64 patients randomized to dextroamphetamine vs placebo (55% men; median age, 66 years; age range, 27-91 years), no overall treatment-associated difference in the mean (SEM) change in Fugl-Meyer motor scores from baseline to 3 months after stroke was noted (-18.65 [2.27] points with dextroamphetamine vs -20.83 [2.94] points with placebo; P = .58). No overall treatment-associated differences in any of the study's secondary measures and no differences in subgroups based on stroke location or baseline severity were found. No adverse events were attributed to study treatments.
Conclusions and relevance: Treatment with dextroamphetamine combined with physical therapy did not improve recovery of motor function compared with placebo combined with physical therapy as assessed 3 months after hemispheric ischemic stroke. The studied treatment regimen was safe.
Trial registration: ClinicalTrials.gov identifier: NCT01905371.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
