

Low skeletal muscle mass is associated with low aerobic capacity and increased mortality risk in patients with coronary heart disease - a CARE CR study
- PMID: 30168241
- PMCID: PMC7379590
- DOI: 10.1111/cpf.12539
Low skeletal muscle mass is associated with low aerobic capacity and increased mortality risk in patients with coronary heart disease - a CARE CR study
Abstract
Background: In patients with chronic heart failure, there is a positive linear relationship between skeletal muscle mass (SMM) and peak oxygen consumption ( O2peak ); an independent predictor of all-cause mortality. We investigated the association between SMM and O2peak in patients with coronary heart disease (CHD) without a diagnosis of heart failure.
Methods: Male patients with CHD underwent maximal cardiopulmonary exercise testing and dual X-ray absorptiometry assessment. O2peak, the ventilatory anaerobic threshold and peak oxygen pulse were calculated. SMM was expressed as appendicular lean mass (lean mass in both arms and legs) and reported as skeletal muscle index (SMI; kg m-2 ), and as a proportion of total body mass (appendicular skeletal mass [ASM%]). Low SMM was defined as a SMI <7·26 kg m-2 , or ASM% <25·72%. Five-year all-cause mortality risk was calculated using the Calibre 5-year all-cause mortality risk score.
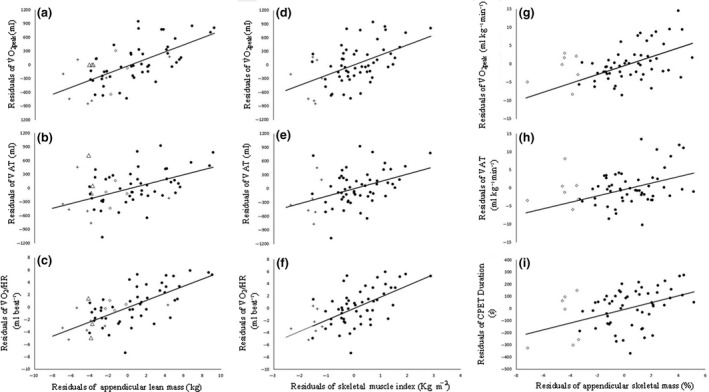
Results: Sixty patients were assessed. Thirteen (21·7%) had low SMM. SMI and ASM% correlated positively with O2peak (r = 0·431 and 0·473, respectively; P<0·001 for both). SMI and ASM% predicted 16·3% and 12·9% of the variance in O2peak , respectively. SMI correlated most closely with peak oxygen pulse (r = 0·58; P<0·001). SMI predicted 40·3% of peak O2 /HR variance. ASM% was inversely associated with 5-year all-cause mortality risk (r = -0·365; P = 0·006).
Conclusion: Skeletal muscle mass was positively correlated with O2peak in patients with CHD. Peak oxygen pulse had the strongest association with SMM. Low ASM% was associated with a higher risk of all-cause mortality. The effects of exercise and nutritional strategies aimed at improving SMM and function in CHD patients should be investigated.
Keywords: cardiorespiratory fitness; coronary disease; sarcopenia; skeletal muscle.
© 2018 The Authors. Clinical Physiology and Functional Imaging published by John Wiley & Sons Ltd on behalf of Scandinavian Society of Clinical Physiology and Nuclear Medicine.
Conflict of interest statement
SN received salary match‐funding from City Health Care Partnership CIC (Hull, UK) during the data collection period of this study. The authors declare no other conflict of interest.
Figures
Similar articles
-
Association between skeletal muscle mass and cardiorespiratory fitness in community-dwelling elderly men.Aging Clin Exp Res. 2019 Jan;31(1):49-57. doi: 10.1007/s40520-018-0987-9. Epub 2018 Jun 18. Aging Clin Exp Res. 2019. PMID: 29916089
-
[Relationships between percentage of skeletal muscle mass and cardiorespiratory fitness in elderly patients with coronary heart disease].Zhonghua Yi Xue Za Zhi. 2018 Mar 20;98(11):831-836. doi: 10.3760/cma.j.issn.0376-2491.2018.11.008. Zhonghua Yi Xue Za Zhi. 2018. PMID: 29609265 Chinese.
-
Relationship between skeletal muscle mass and cardiac function during exercise in community-dwelling older adults.ESC Heart Fail. 2017 Nov;4(4):409-416. doi: 10.1002/ehf2.12158. Epub 2017 Apr 10. ESC Heart Fail. 2017. PMID: 29154420 Free PMC article.
-
Sarcopenia and chronic liver diseases.Expert Rev Gastroenterol Hepatol. 2018 Dec;12(12):1229-1244. doi: 10.1080/17474124.2018.1534586. Epub 2018 Oct 16. Expert Rev Gastroenterol Hepatol. 2018. PMID: 30791794 Review.
-
Roles of periodic breathing and isocapnic buffering period during exercise in heart failure.Eur J Prev Cardiol. 2020 Dec;27(2_suppl):19-26. doi: 10.1177/2047487320952029. Eur J Prev Cardiol. 2020. PMID: 33238742 Free PMC article. Review.
Cited by
-
Sarcopenia and coronary heart disease synergistically increase the risk of new onset depressive symptoms in older adults.BMC Geriatr. 2021 Dec 24;21(1):731. doi: 10.1186/s12877-021-02710-z. BMC Geriatr. 2021. PMID: 34952569 Free PMC article.
-
Relationship Between Number of Cardiac Rehabilitation Exercise Training Sessions, Muscle Mass, and Cardiorespiratory Fitness in Rural Elderly Patients with Coronary Artery Disease.J Multidiscip Healthc. 2023 Nov 7;16:3309-3318. doi: 10.2147/JMDH.S434056. eCollection 2023. J Multidiscip Healthc. 2023. PMID: 37954469 Free PMC article.
-
Sarcopenia during COVID-19 lockdown restrictions: long-term health effects of short-term muscle loss.Geroscience. 2020 Dec;42(6):1547-1578. doi: 10.1007/s11357-020-00272-3. Epub 2020 Oct 1. Geroscience. 2020. PMID: 33001410 Free PMC article. Review.
-
Association between sarcopenia-related traits and cardiovascular diseases: a bi-directional Mendelian randomization study.Front Endocrinol (Lausanne). 2023 Oct 13;14:1237971. doi: 10.3389/fendo.2023.1237971. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37900136 Free PMC article.
-
The commonly used antibiotic streptomycin reduces protein synthesis and differentiation in cultured C2C12 myotubes.Physiol Rep. 2025 Jun;13(12):e70353. doi: 10.14814/phy2.70353. Physiol Rep. 2025. PMID: 40526031 Free PMC article.
References
-
- ACSM . ACSM's Guidelines for Exercise Testing and Prescription (2017). Wolters Kluwer/Lippincott Williams & Wilkins Health, Philadelphia.
-
- American Thoracic Society/American College of Chest Physicians . ATS/ACCP Statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med (2003); 167: 211. - PubMed
-
- Balady GJ, Arena R, Sietsema K, et al Clinician's guide to cardiopulmonary exercise testing in adults: a scientific statement from the American Heart Association. Circulation (2010); 122: 191–225. - PubMed
-
- Bassett D, Howley E. Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med Sci Sports Exerc (2000); 32: 70–84. - PubMed
-
- Beaver WL, Wasserman K, Whipp BJ. A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol (1986); 60: 2020–2027. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
