

Relationship between changing patient-reported outcomes and subsequent clinical events in patients with chronic heart failure: insights from HF-ACTION
- PMID: 30168635
- PMCID: PMC6333485
- DOI: 10.1002/ejhf.1299
Relationship between changing patient-reported outcomes and subsequent clinical events in patients with chronic heart failure: insights from HF-ACTION
Abstract
Aims: A 5-point change in the Kansas City Cardiomyopathy Questionnaire (KCCQ) is commonly considered to be a clinically significant difference in health status in patients with heart failure. We evaluated how the magnitude of change relates to subsequent clinical outcomes.
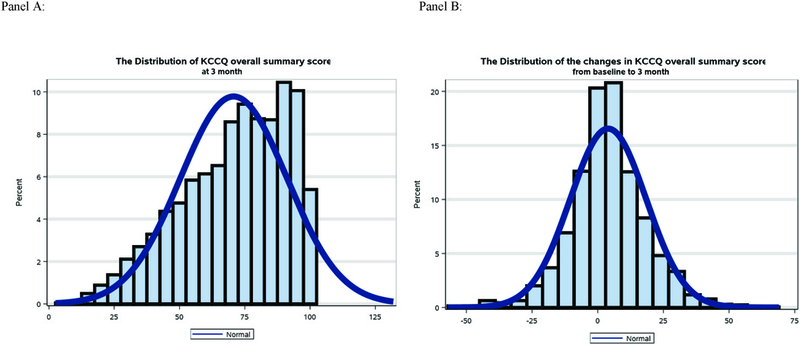
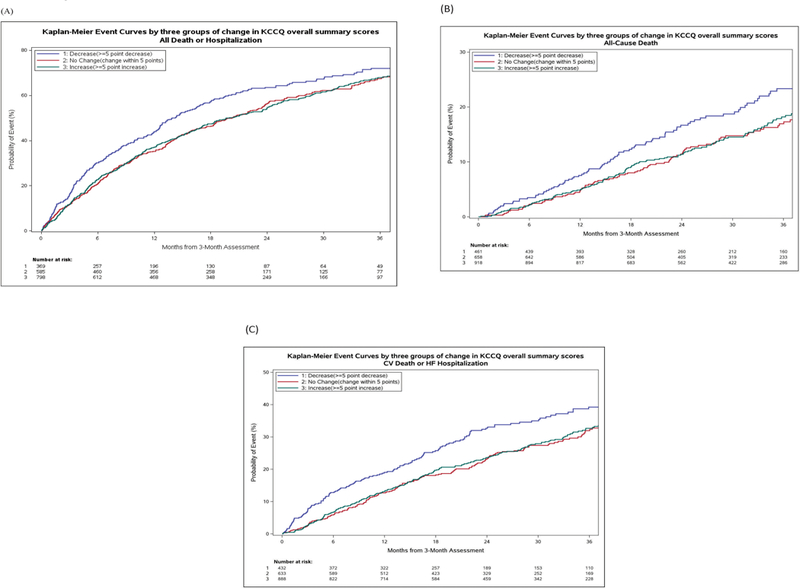
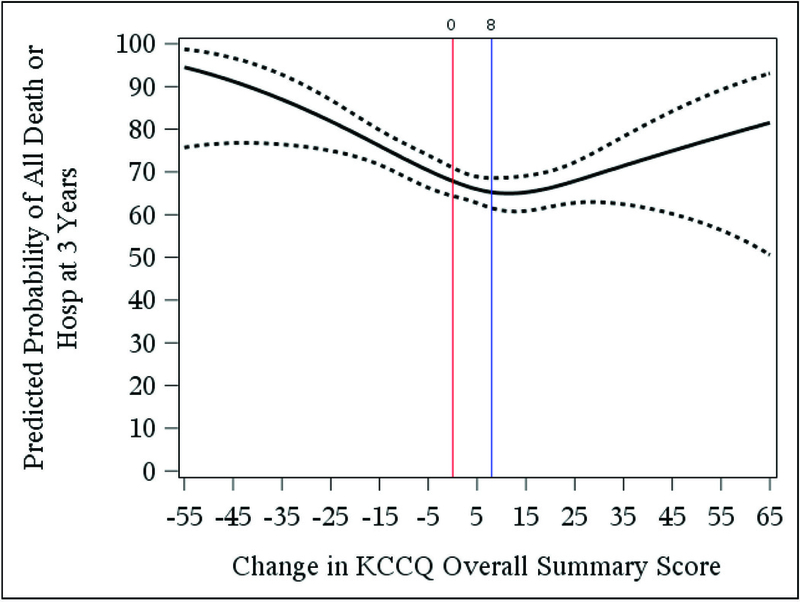
Methods and results: Using data from the HF-ACTION trial of exercise training in chronic heart failure (n = 2331), we used multivariable Cox regression with piecewise linear splines to examine the relationship between change in KCCQ overall summary score from baseline to 3 months (range 0-100; higher scores reflect better health status) and subsequent all-cause mortality/hospitalization. Among 2038 patients with KCCQ data at the 3-month visit, KCCQ scores increased from baseline by ≥5 points for 45%, scores decreased by ≥5 points for 23%, and scores changed by <5 points for the remaining 32% of patients. There was a non-linear relationship between change in KCCQ and outcomes. Worsening health status was associated with increased all-cause mortality/hospitalization (adjusted hazard ratio 1.07 per 5-point KCCQ decline; 95% confidence interval 1.03-1.12; P < 0.001). In contrast, improving health status, up to an 8-point increase in KCCQ, was associated with decreased all-cause mortality/hospitalization (adjusted hazard ratio 0.93 per 5-point increase; 95% confidence interval 0.90-0.97; P < 0.001). Additional improvements in health status beyond an 8-point increase in KCCQ was not associated with all-cause death or hospitalization (P = 0.42).
Conclusion: In patients with heart failure, small changes in KCCQ are associated with changing future risk, but more research will be necessary to understand how different magnitudes of improving health status affect outcomes.
Trial registration: ClinicalTrials.gov NCT00047437.
Keywords: Health status; Patient-reported outcomes; Quality of life.
© 2018 The Authors. European Journal of Heart Failure © 2018 European Society of Cardiology.
Conflict of interest statement
Disclosures:
The authors report no relevant conflicts of interest or relationships with industry.
Figures
Comment in
-
Patient-reported and morbidity-mortality endpoints: can one have the best of both worlds?Eur J Heart Fail. 2019 Jan;21(1):71-73. doi: 10.1002/ejhf.1317. Epub 2018 Oct 2. Eur J Heart Fail. 2019. PMID: 30280452 No abstract available.
References
-
- Croog SH, Levine S, Testa MA, Brown B, Bulpitt CJ, Jenkins CD, Klerman GL, Williams GH. The effects of antihypertensive therapy on the quality of life. N Engl J Med 1986;314(26):1657–64. - PubMed
-
- Cleary PD, Epstein AM, Oster G, Morrissey GS, Stason WB, Debussey S, Plachetka J, Zimmerman M. Health-related quality of life among patients undergoing percutaneous transluminal coronary angioplasty. Med Care 1991;29(10):939–50. - PubMed
-
- Lesperance F, Frasure-Smith N, Koszycki D, Laliberte MA, van Zyl LT, Baker B, Swenson JR, Ghatavi K, Abramson BL, Dorian P, Guertin MC, Investigators C. Effects of citalopram and interpersonal psychotherapy on depression in patients with coronary artery disease: the Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy (CREATE) trial. JAMA 2007;297(4):367–79. - PubMed
-
- Flynn KE, Pina IL, Whellan DJ, Lin L, Blumenthal JA, Ellis SJ, Fine LJ, Howlett JG, Keteyian SJ, Kitzman DW, Kraus WE, Miller NH, Schulman KA, Spertus JA, O’Connor CM, Weinfurt KP, Investigators H-A. Effects of exercise training on health status in patients with chronic heart failure: HF-ACTION randomized controlled trial. JAMA 2009;301(14):1451–9. - PMC - PubMed
-
- McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, Rouleau JL, Shi VC, Solomon SD, Swedberg K, Zile MR, Investigators P-H, Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014;371(11):993–1004. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
