

Residual Cochlear Function in Adults and Children Receiving Cochlear Implants: Correlations With Speech Perception Outcomes
- PMID: 30169463
- PMCID: PMC6533622
- DOI: 10.1097/AUD.0000000000000630
Residual Cochlear Function in Adults and Children Receiving Cochlear Implants: Correlations With Speech Perception Outcomes
Erratum in
-
Residual Cochlear Function in Adults and Children Receiving Cochlear Implants: Correlations With Speech Perception Outcomes: Erratum.Ear Hear. 2019 Jul/Aug;40(4):1034. doi: 10.1097/AUD.0000000000000757. Ear Hear. 2019. PMID: 31241600 No abstract available.
Abstract
Objectives: Variability in speech perception outcomes with cochlear implants remains largely unexplained. Recently, electrocochleography, or measurements of cochlear potentials in response to sound, has been used to assess residual cochlear function at the time of implantation. Our objective was to characterize the potentials recorded preimplantation in subjects of all ages, and evaluate the relationship between the responses, including a subjective estimate of neural activity, and speech perception outcomes.
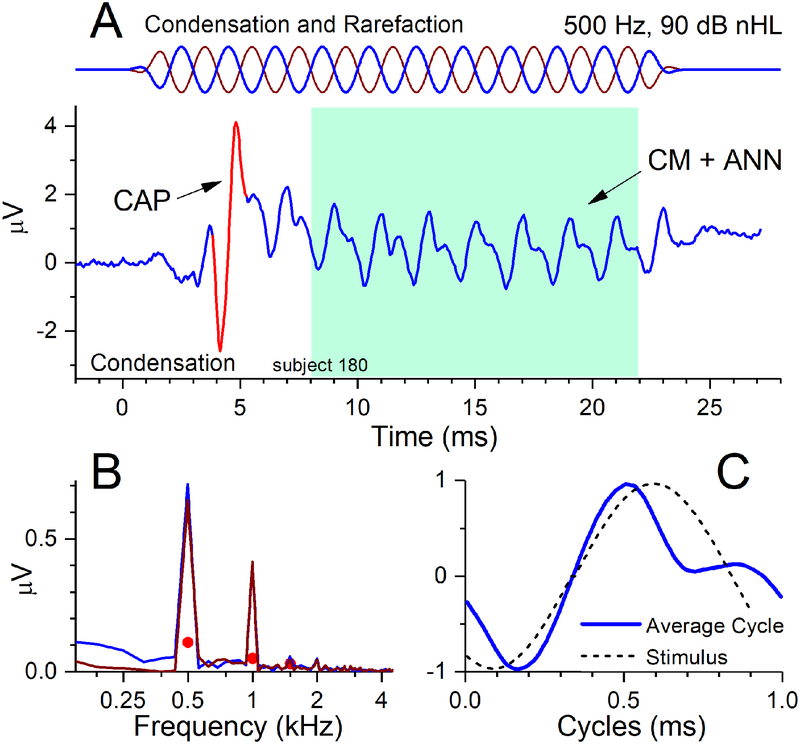
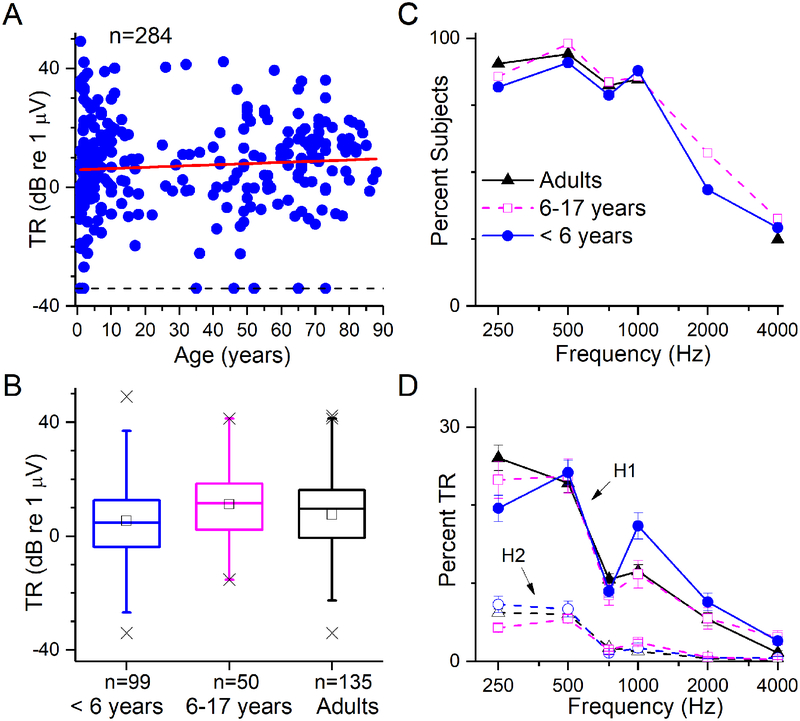
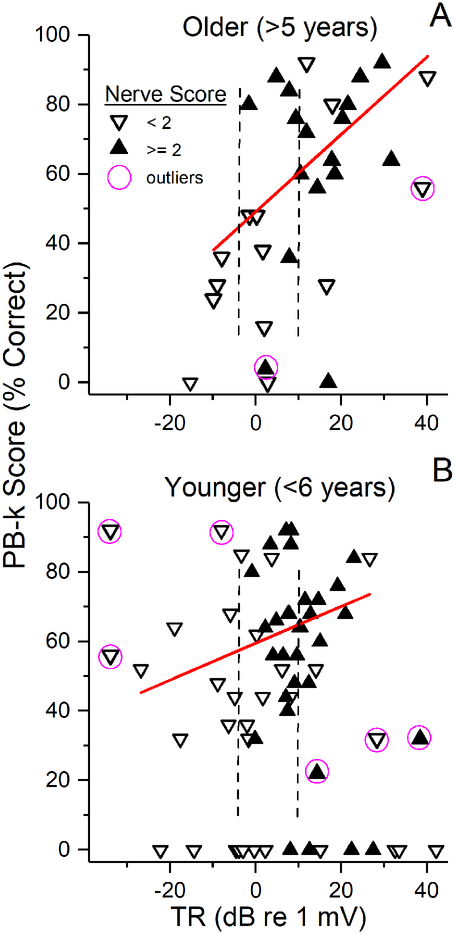
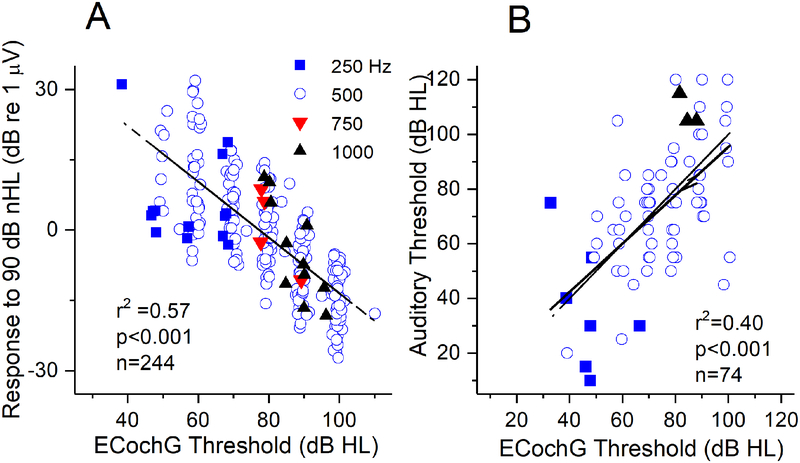
Design: Electrocochleography was recorded in a prospective cohort of 284 candidates for cochlear implant at University of North Carolina (10 months to 88 years of ages). Measurement of residual cochlear function called the "total response" (TR), which is the sum of magnitudes of spectral components in response to tones of different stimulus frequencies, was obtained for each subject. The TR was then related to results on age-appropriate monosyllabic word score tests presented in quiet. In addition to the TR, the electrocochleography results were also assessed for neural activity in the forms of the compound action potential and auditory nerve neurophonic.
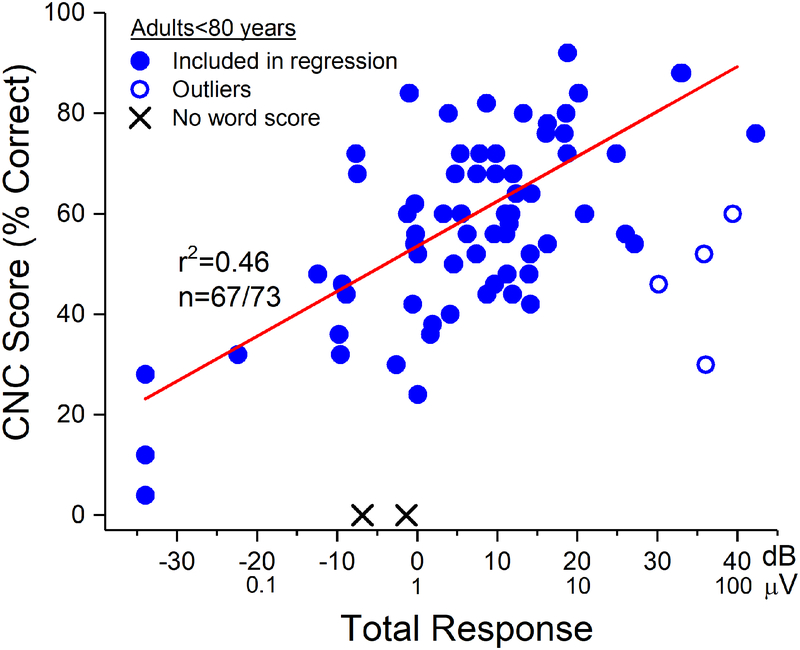
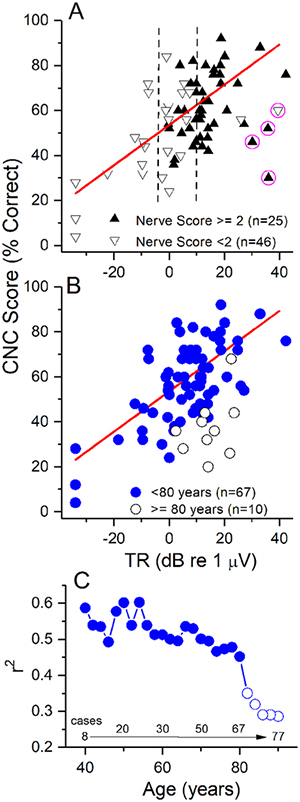
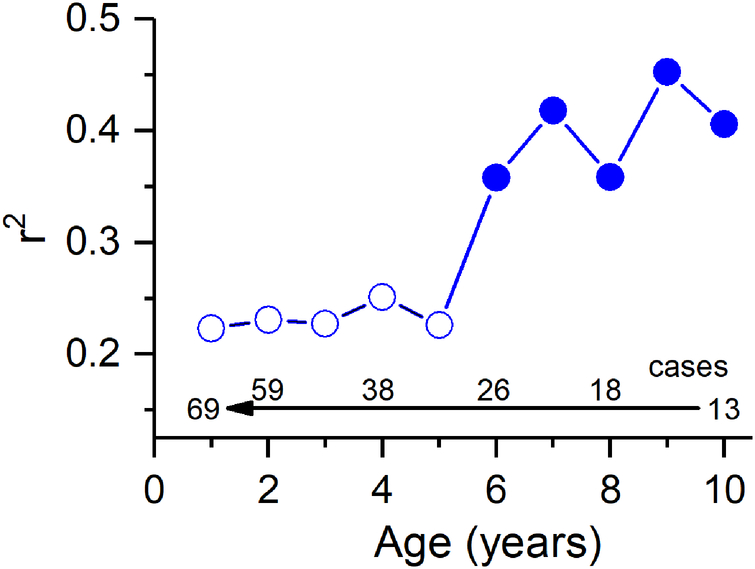
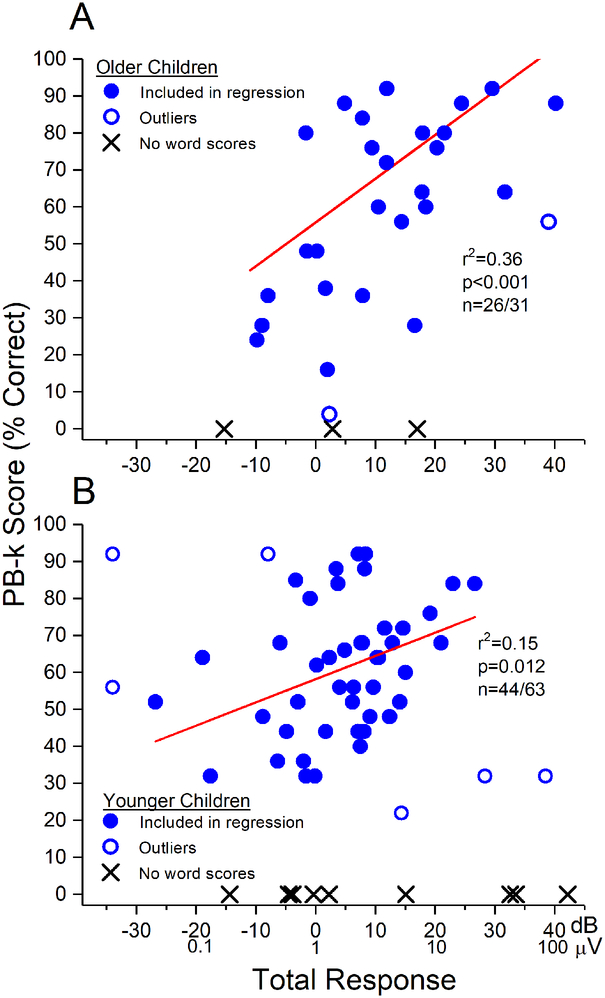
Results: The TR magnitude ranged from a barely detectable response of about 0.02 µV to more than 100 µV. In adults (18 to 79 years old), the TR accounted for 46% of variability in speech perception outcome by linear regression (r = 0.46; p < 0.001). In children between 6 and 17 years old, the variability accounted for was 36% (p < 0.001). In younger children, the TR accounted for less of the variability, 15% (p = 0.012). Subjects over 80 years old tended to perform worse for a given TR than younger adults at the 6-month testing interval. The subjectively assessed neural activity did not increase the information compared with the TR alone, which is primarily composed of the cochlear microphonic produced by hair cells.
Conclusions: The status of the auditory periphery, particularly of hair cells rather than neural activity, accounts for a large fraction of variability in speech perception outcomes in adults and older children. In younger children, the relationship is weaker, and the elderly differ from other adults. This simple measurement can be applied with high throughput so that peripheral status can be assessed to help manage patient expectations, create individually-tailored treatment plans, and identify subjects performing below expectations based on residual cochlear function.
Conflict of interest statement
Conflicts of Interest and Source of Funding
Dr. Fitzpatrick, Dr. Adunka, Dr. Buchman, Dr. Teagle, Dr. Pillsbury and Dr. Brown have consulting arrangements and research projects with MED-EL, Cochlear Corp and Advanced Bionics. This project was funded by NIH through NIDCD (5T32DC005360-12 and 1-F30-DC-015168-01A1) and by a research contract with MED-EL Corporation.
Figures
References
-
- Acharya AN, Tavora-Vieira D, Rajan GP (2016). Using the Implant Electrode Array to Conduct Real-time Intraoperative Hearing Monitoring During Pediatric Cochlear Implantation: Preliminary Experiences. Otol Neurotol, 37, e148–153. - PubMed
-
- Adunka OF, Dillon MT, Adunka MC, et al. (2013). Hearing preservation and speech perception outcomes with electric-acoustic stimulation after 12 months of listening experience. Laryngoscope, 123, 2509–2515. - PubMed
-
- Ahmad FI, Demason CE, HF BT, et al. (2012). Cochlear implantation in children with postlingual hearing loss. Laryngoscope. - PubMed
-
- Aminpour S, Tinling SP, Brodie HA (2005). Role of tumor necrosis factor-alpha in sensorineural hearing loss after bacterial meningitis. Otol Neurotol, 26, 602–609. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
