

Prophylactic lactoferrin for preventing late-onset sepsis and necrotizing enterocolitis in preterm infants: A PRISMA-compliant systematic review and meta-analysis
- PMID: 30170397
- PMCID: PMC6392939
- DOI: 10.1097/MD.0000000000011976
Prophylactic lactoferrin for preventing late-onset sepsis and necrotizing enterocolitis in preterm infants: A PRISMA-compliant systematic review and meta-analysis
Abstract
Background: Currently, prophylactic use of drugs to promote a healthy gut microbiota and immune system in preterm infants is hot debated, among which lactoferrin is a promising supplementation. However, the effect and safety of lactoferrin to prevent late-onset sepsis (LOS) and necrotizing enterocolitis (NEC) in preterm infants remains controversial.
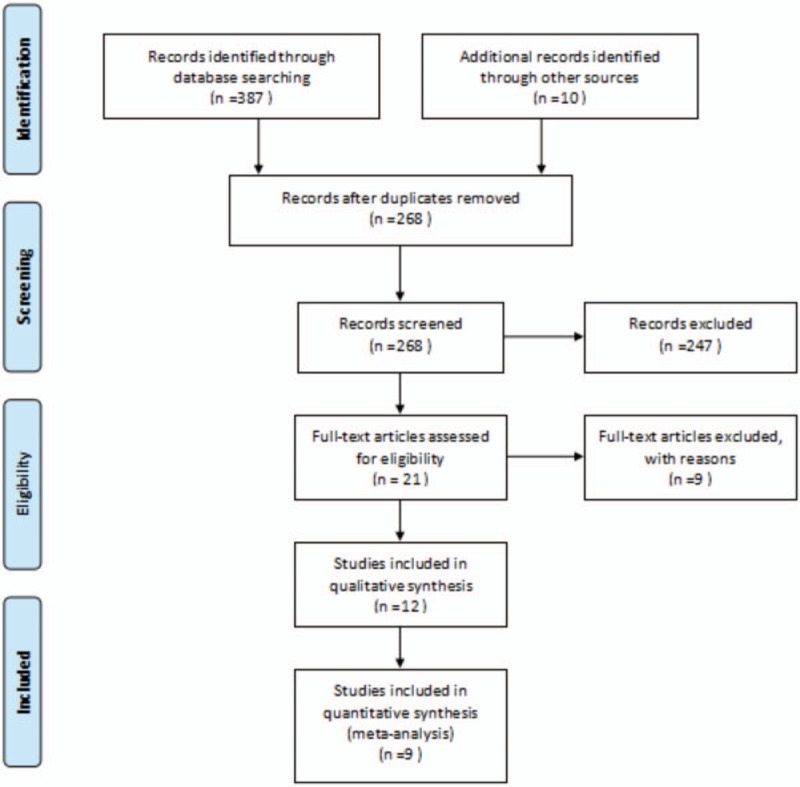
Methods: Databases including Medline, Ovid-Embase, The Cochrane Library, CBM, CNKI, and VIP database of Chinese Journal were searched to collect randomized controlled trials (RCTs) about lactoferrin for preventing LOS and NEC in preterm infants. Languages of included RCTs were restricted to English and Chinese. Meta-analysis was conducted by Rev Man 5.3 software. The Mantel-Haenszel method with random-effects model was used to calculate pooled relative risks (RRs) and 95% confidence intervals (CIs).
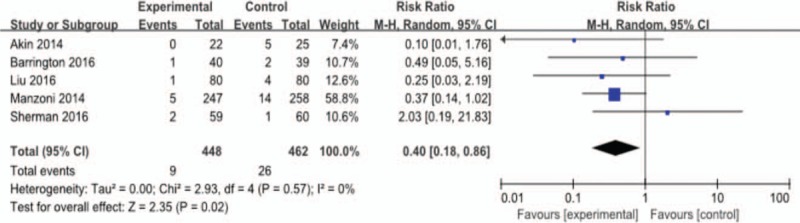
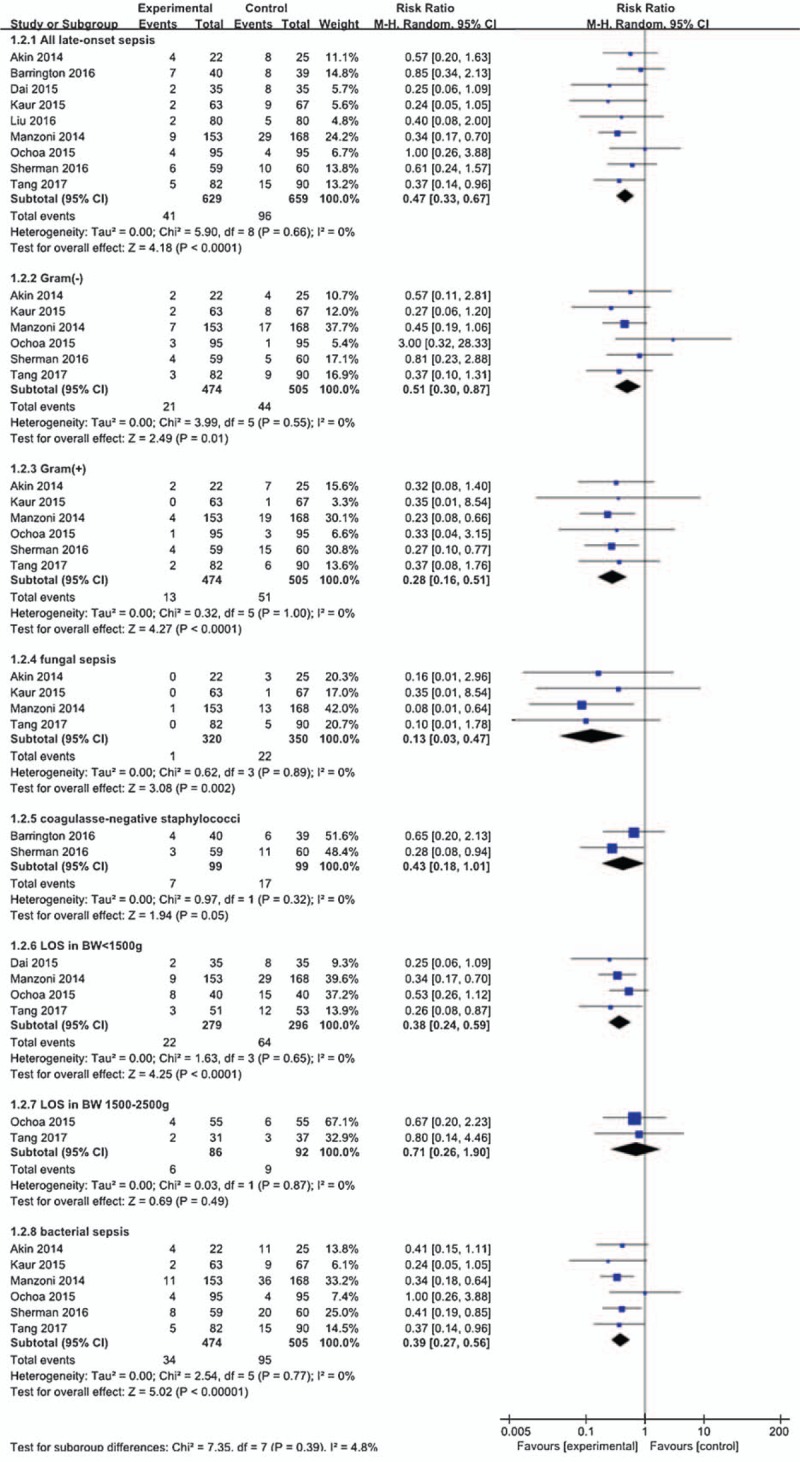
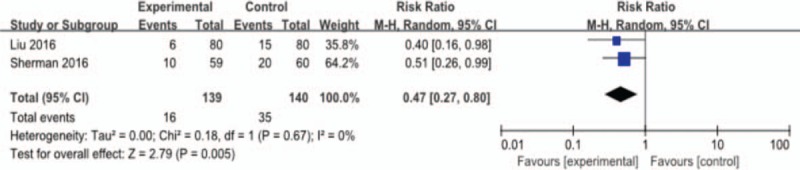
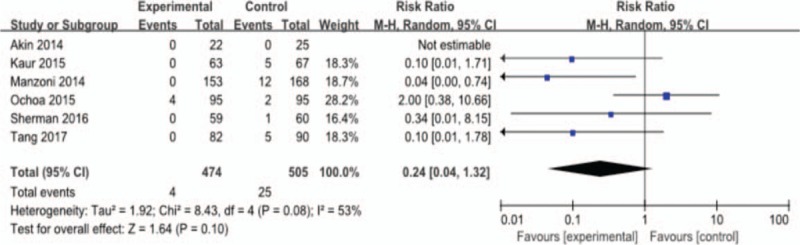
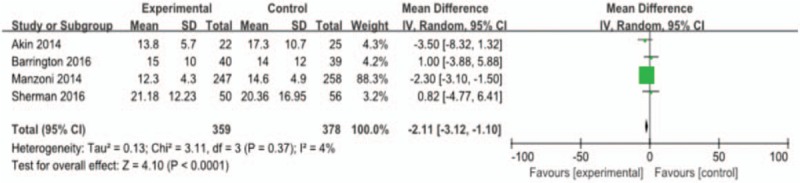
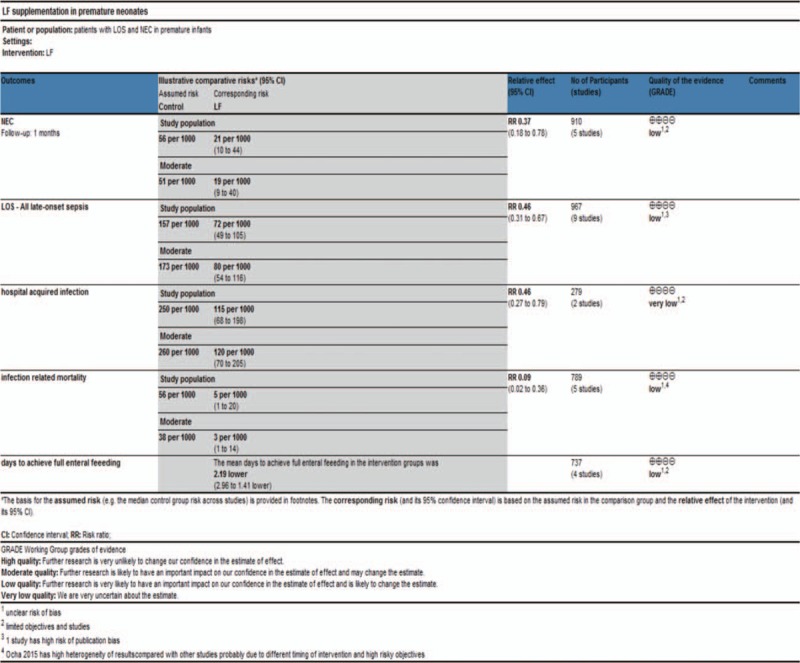
Results: A total of 9 RCTs, involving 1834 patients, were included. Pooled analysis showed that prophylactic lactoferrin could significantly reduce the incidence all culture-proven LOS (41/629 [6.5%] vs 96/659 [15.3%]; RR 0.47; 95% CI 0.33-0.67; P < .01) and NEC (stage II or more) (9/448 [2.0%] vs 26/462 [5.6%]; RR 0.40; 95% CI 0.18-0.86; P < .01). Lactoferrin was also associated with a significantly decreased hospital-acquired infection (16/139 [11.5%] vs 35/140 [25%]; RR 0.47; 95% CI 0.27-0.80; P < .01); and infection-related mortality (4/474 [0.8%] vs 25/505 [4.9%]; RR 0.24; 95% CI 0.04-1.32; P < .01, I = 53%). Lactoferrin could shorten time to reach full enteral feeding (weighted mean difference [WMD] = -2.11, 95% CI -3.12 to -1.10; P < .01) and showed a decreasing trend of duration of hospitalization (WMD = -1.69, 95% CI -6.87 to 3.50; P < .01; I = 95%). Lactoferrin did not have a significant effect on all-cause mortality (22/625 [3.5%] vs 35/647 [5.4%]; RR 0.70; 95% CI 0.38-1.30; P = .16; I = 13%). None of the included trials reported any confirmed adverse effects caused by the supplemented lactoferrin or probiotics.
Conclusion: Current evidence indicates that lactoferrin could significantly reduce the incidence of NEC and LOS, and decrease the risk of hospital-acquired infection and infection-related mortality in premature infants without obvious adverse effects.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Liu L, Johnson HL, Cousens S, et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet 2012;379:2151–61. - PubMed
-
- Stoll BJ, Hansen N, Fanaroff AA, et al. Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Pediatrics 2002;110:285–91. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
