

Assessing the sensitivity of placental growth factor and soluble fms-like tyrosine kinase 1 at 36 weeks' gestation to predict small-for-gestational-age infants or late-onset preeclampsia: a prospective nested case-control study
- PMID: 30170567
- PMCID: PMC6119271
- DOI: 10.1186/s12884-018-1992-x
Assessing the sensitivity of placental growth factor and soluble fms-like tyrosine kinase 1 at 36 weeks' gestation to predict small-for-gestational-age infants or late-onset preeclampsia: a prospective nested case-control study
Abstract
Background: Fetal growth restriction is a disorder of placental dysfunction with three to four-fold increased risk of stillbirth. Fetal growth restriction has pathophysiological features in common with preeclampsia. We hypothesised that angiogenesis-related factors in maternal plasma, known to predict preeclampsia, may also detect fetal growth restriction at 36 weeks' gestation. We therefore set out to determine the diagnostic performance of soluble fms-like tyrosine kinase 1 (sFlt-1), placental growth factor (PlGF), and the sFlt-1:PlGF ratio, measured at 36 weeks' gestation, in identifying women who subsequently give birth to small-for-gestational-age (SGA; birthweight <10th centile) infants. We also aimed to validate the predictive performance of the analytes for late-onset preeclampsia in a large independent, prospective cohort.
Methods: A nested 1:2 case-control study was performed including 102 cases of SGA infants and a matched group of 207 controls; and 39 cases of preeclampsia. We determined the diagnostic performance of each angiogenesis-related factor, and of their ratio, to detect SGA infants or preeclampsia, for a predetermined 10% false positive rate.
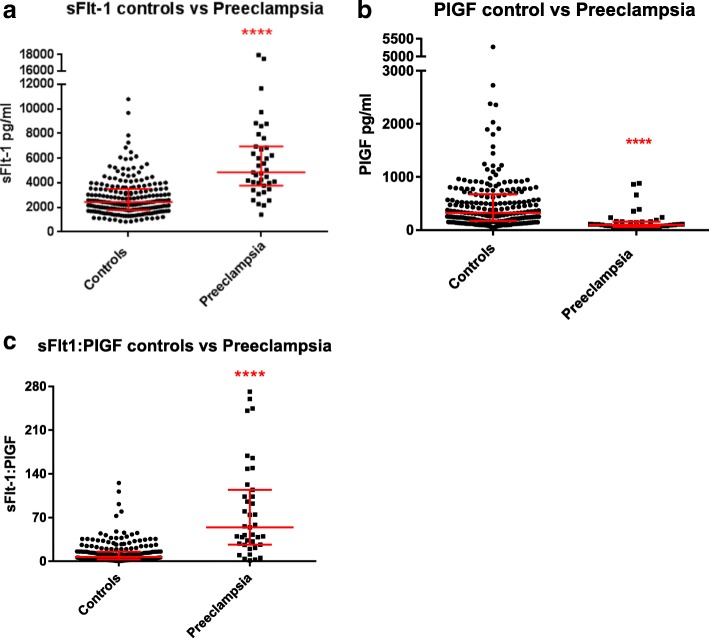
Results: Median plasma levels of PlGF at 36 weeks' gestation were significantly lower in women who subsequently had SGA newborns (178.5 pg/ml) compared to normal birthweight controls (326.7 pg/ml, p < 0.0001). sFlt-1 was also higher among SGA cases, but this was not significant after women with concurrent preeclampsia were excluded. The sensitivity of PlGF to predict SGA infants was 28.8% for a 10% false positive rate. The sFlt-1:PlGF ratio demonstrated better sensitivity for preeclampsia than either analyte alone, detecting 69.2% of cases for a 10% false positive rate.
Conclusions: Plasma PlGF at 36 weeks' gestation is significantly lower in women who subsequently deliver a SGA infant. While the sensitivity and specificity of PlGF currently limit clinical translation, our findings support a blood-based biomarker approach to detect late-onset fetal growth restriction. Thirty-six week sFlt-1:PlGF ratio predicts 69.2% of preeclampsia cases, and could be a useful screening test to triage antenatal surveillance.
Keywords: Biomarker; Fetal growth restriction; Late-onset; Placental growth factor; Preeclampsia; Small-for-gestational-age; Soluble fms-like tyrosine kinase 1.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Mercy Health Research Ethics Committee (Ethics Approval Number R14/12) and written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



Similar articles
-
Soluble fms-like tyrosine kinase to placental growth factor ratio in different stages of early-onset fetal growth restriction and small for gestational age.Acta Obstet Gynecol Scand. 2021 Jan;100(1):119-128. doi: 10.1111/aogs.13978. Epub 2020 Sep 14. Acta Obstet Gynecol Scand. 2021. PMID: 32860218
-
Placental growth factor and soluble fms-like tyrosine kinase-1 are useful markers for the prediction of preeclampsia but not for small for gestational age neonates: a longitudinal study.Eur J Obstet Gynecol Reprod Biol. 2013 Dec;171(2):225-30. doi: 10.1016/j.ejogrb.2013.08.040. Epub 2013 Sep 4. Eur J Obstet Gynecol Reprod Biol. 2013. PMID: 24035323
-
Prediction of small-for-gestational-age neonates: screening by placental growth factor and soluble fms-like tyrosine kinase-1 at 35-37 weeks.Ultrasound Obstet Gynecol. 2015 Aug;46(2):191-7. doi: 10.1002/uog.14862. Epub 2015 Jun 18. Ultrasound Obstet Gynecol. 2015. PMID: 25825848
-
Combining Biomarkers to Predict Pregnancy Complications and Redefine Preeclampsia: The Angiogenic-Placental Syndrome.Hypertension. 2020 Apr;75(4):918-926. doi: 10.1161/HYPERTENSIONAHA.119.13763. Epub 2020 Feb 17. Hypertension. 2020. PMID: 32063058 Free PMC article. Review.
-
Biochemical tests of placental function versus ultrasound assessment of fetal size for stillbirth and small-for-gestational-age infants.Cochrane Database Syst Rev. 2019 May 14;5(5):CD012245. doi: 10.1002/14651858.CD012245.pub2. Cochrane Database Syst Rev. 2019. PMID: 31087568 Free PMC article.
Cited by
-
Slowing fetal growth velocity from the mid-trimester may signal increased risks of perinatal morbidity and mortality: a retrospective cohort study.BMC Med. 2025 May 28;23(1):298. doi: 10.1186/s12916-025-04117-8. BMC Med. 2025. PMID: 40437548 Free PMC article.
-
Adverse Neonatal Outcome of Pregnancies Complicated by Preeclampsia.Biomedicines. 2022 Aug 22;10(8):2048. doi: 10.3390/biomedicines10082048. Biomedicines. 2022. PMID: 36009597 Free PMC article.
-
"Screening for small-for-gestational age neonates at early third trimester in a high-risk population for preeclampsia".BMC Pregnancy Childbirth. 2020 Sep 25;20(1):563. doi: 10.1186/s12884-020-03167-5. BMC Pregnancy Childbirth. 2020. PMID: 32988372 Free PMC article.
-
Follicular fluid PlGF and IVF/ICSI outcomes among PCOS and normo-ovulatory women using different controlled hyperstimulation protocols: A prospective case-control study.Ann Med Surg (Lond). 2022 Jun 25;79:104096. doi: 10.1016/j.amsu.2022.104096. eCollection 2022 Jul. Ann Med Surg (Lond). 2022. PMID: 35860057 Free PMC article.
-
Maternal serum soluble fms-like tyrosine kinase-1-to-placental growth factor ratio distinguishes growth-restricted from non-growth-restricted small-for-gestational-age fetuses.AJOG Glob Rep. 2024 Jan 9;4(1):100302. doi: 10.1016/j.xagr.2023.100302. eCollection 2024 Feb. AJOG Glob Rep. 2024. PMID: 38318268 Free PMC article.
References
-
- Mendez-Figueroa H, Truong VT, Pedroza C, Khan AM, Chauhan SP. Small-for-gestational-age infants among uncomplicated pregnancies at term: a secondary analysis of 9 maternal-fetal medicine units network studies. Am J Obstet Gynecol. 2016;215:628.e621–628.e627. doi: 10.1016/j.ajog.2016.06.043. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
