

Ganglionic Antibody Level as a Predictor of Severity of Autonomic Failure
- PMID: 30170741
- PMCID: PMC6173625
- DOI: 10.1016/j.mayocp.2018.05.033
Ganglionic Antibody Level as a Predictor of Severity of Autonomic Failure
Abstract
Objective: To assess antibody level as a test of autonomic failure (AF) associated with ganglionic nicotinic acetylcholine receptor antibody (AChR-Ab) autoimmunity.
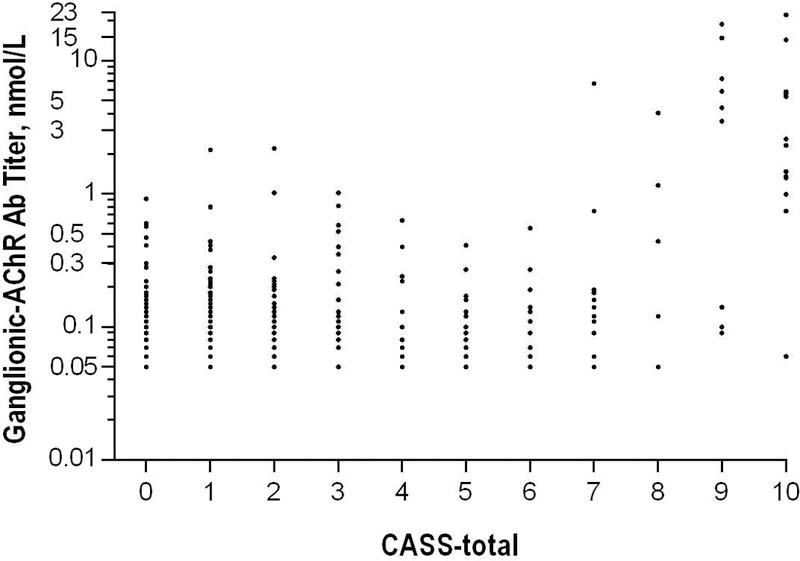
Patients and methods: We searched the Mayo Clinic laboratory database of 926 ganglionic AChR-Ab-seropositive patients seen at our institution between October 1, 1997, and April 1, 2015, for initial level of 0.05 nmol/L or higher and contemporaneous autonomic reflex screen (standardized evaluation of adrenergic, cardiovagal, and sudomotor functions) from which Composite Autonomic Scoring Scale (CASS) scores could be calculated.
Results: Of 289 patients who met inclusion criteria, 163 (56.4%) were women, median age was 54 years (range, 10-87 years), median antibody level was 0.11 nmol/L (range, 0.05-22.10 nmol/L), and median CASS total score was 2.0 (range, 0-10). Using receiver operating characteristic curve analysis, a level above 0.40 nmol/L predicted severe AF (CASS score, ≥7) with 92% specificity and 56% sensitivity. For at least moderate AF (CASS score ≥4 and anhidrosis ≥25%), a level of at least 0.20 nmol/L had 80% specificity and 59% sensitivity. Levels below 0.20 nmol/L were not predictive of the presence or absence of AF. For predicting orthostatic hypotension, ganglionic AChR-Ab level had excellent specificity above 0.4 nmol/L but lacked sensitivity. Autoantibodies to additional targets were present in 61 patients (21.1%).
Conclusion: Ganglionic AChR-Ab level of at least 0.40 nmol/L is a moderately sensitive and highly specific marker for severe AF, as is a level of at least 0.20 nmol/L for moderate AF if CASS score is coupled with anhidrosis of 25% or more, among patients with suspected ganglionic AChR-Ab autoimmune autonomic ganglionopathy. Antibody levels of less than 0.20 nmol/L have little clinical importance in the absence of clinical AF.
Copyright © 2018 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Young RR, Asbury AK, Adams RD, Corbett JL. Pure pan-dysautonomia with recovery. Trans Am Neurol Assoc 1969;94:355–357. - PubMed
-
- Vernino S, Adamski J, Kryzer TJ, Fealey RD, Lennon VA. Neuronal nicotinic ACh receptor antibody in subacute autonomic neuropathy and cancer-related syndromes. Neurology 1998;50(6):1806–1813. - PubMed
-
- Vernino S, Low PA, Fealey RD, Stewart JD, Farrugia G, Lennon VA. Autoantibodies to ganglionic acetylcholine receptors in autoimmune autonomic neuropathies. N Engl J Med 2000;343(12):847–855. - PubMed
-
- Gibbons CH, Freeman R. Antibody titers predict clinical features of autoimmune autonomic ganglionopathy. Auton Neurosci 2009;146(1–2):8–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
