

Non-invasive detection of coronary inflammation using computed tomography and prediction of residual cardiovascular risk (the CRISP CT study): a post-hoc analysis of prospective outcome data
- PMID: 30170852
- PMCID: PMC6137540
- DOI: 10.1016/S0140-6736(18)31114-0
Non-invasive detection of coronary inflammation using computed tomography and prediction of residual cardiovascular risk (the CRISP CT study): a post-hoc analysis of prospective outcome data
Abstract
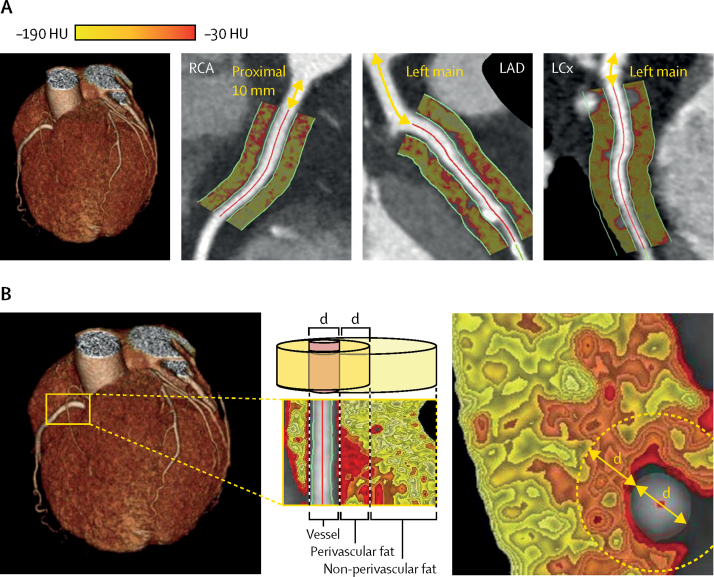
Background: Coronary artery inflammation inhibits adipogenesis in adjacent perivascular fat. A novel imaging biomarker-the perivascular fat attenuation index (FAI)-captures coronary inflammation by mapping spatial changes of perivascular fat attenuation on coronary computed tomography angiography (CTA). However, the ability of the perivascular FAI to predict clinical outcomes is unknown.
Methods: In the Cardiovascular RISk Prediction using Computed Tomography (CRISP-CT) study, we did a post-hoc analysis of outcome data gathered prospectively from two independent cohorts of consecutive patients undergoing coronary CTA in Erlangen, Germany (derivation cohort) and Cleveland, OH, USA (validation cohort). Perivascular fat attenuation mapping was done around the three major coronary arteries-the proximal right coronary artery, the left anterior descending artery, and the left circumflex artery. We assessed the prognostic value of perivascular fat attenuation mapping for all-cause and cardiac mortality in Cox regression models, adjusted for age, sex, cardiovascular risk factors, tube voltage, modified Duke coronary artery disease index, and number of coronary CTA-derived high-risk plaque features.
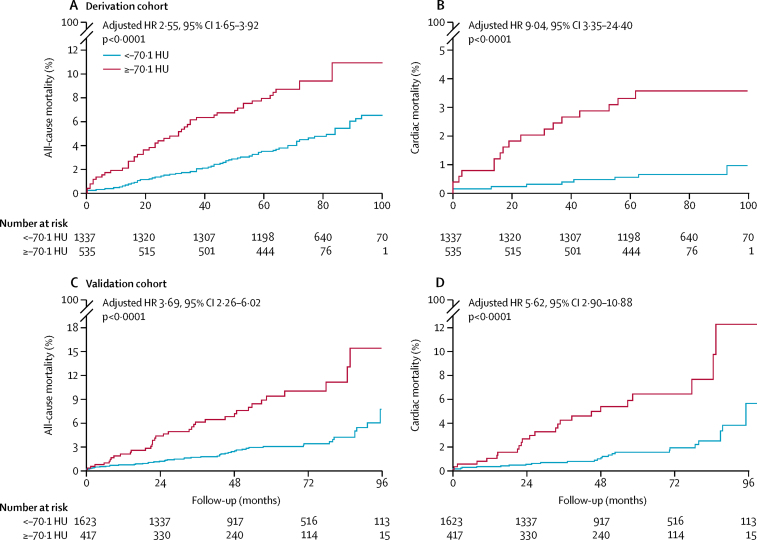
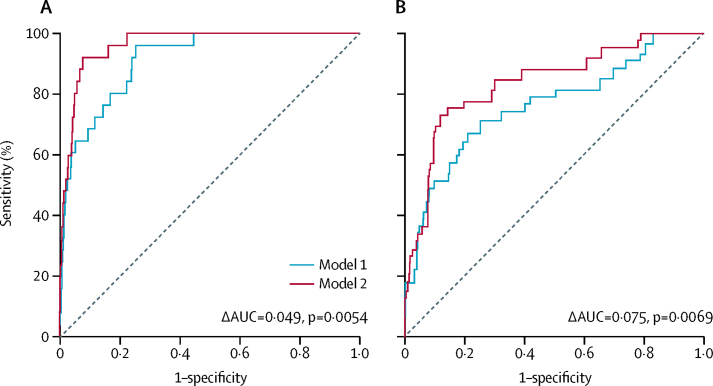
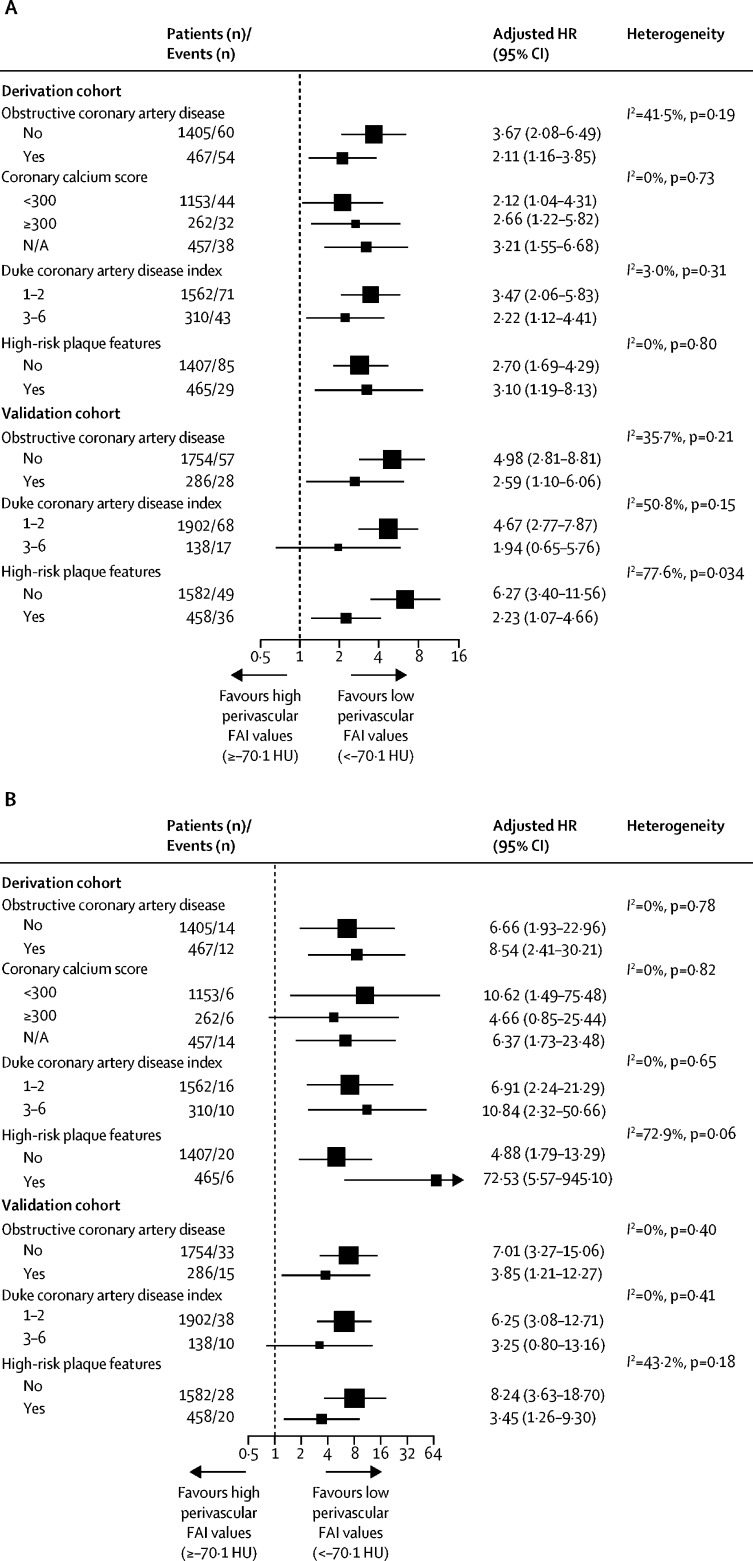
Findings: Between 2005 and 2009, 1872 participants in the derivation cohort underwent coronary CTA (median age 62 years [range 17-89]). Between 2008 and 2016, 2040 patients in the validation cohort had coronary CTA (median age 53 years [range 19-87]). Median follow-up was 72 months (range 51-109) in the derivation cohort and 54 months (range 4-105) in the validation cohort. In both cohorts, high perivascular FAI values around the proximal right coronary artery and left anterior descending artery (but not around the left circumflex artery) were predictive of all-cause and cardiac mortality and correlated strongly with each other. Therefore, the perivascular FAI measured around the right coronary artery was used as a representative biomarker of global coronary inflammation (for prediction of cardiac mortality, hazard ratio [HR] 2·15, 95% CI 1·33-3·48; p=0·0017 in the derivation cohort, and 2·06, 1·50-2·83; p<0·0001 in the validation cohort). The optimum cutoff for the perivascular FAI, above which there is a steep increase in cardiac mortality, was ascertained as -70·1 Hounsfield units (HU) or higher in the derivation cohort (HR 9·04, 95% CI 3·35-24·40; p<0·0001 for cardiac mortality; 2·55, 1·65-3·92; p<0·0001 for all-cause mortality). This cutoff was confirmed in the validation cohort (HR 5·62, 95% CI 2·90-10·88; p<0·0001 for cardiac mortality; 3·69, 2·26-6·02; p<0·0001 for all-cause mortality). Perivascular FAI improved risk discrimination in both cohorts, leading to significant reclassification for all-cause and cardiac mortality.
Interpretation: The perivascular FAI enhances cardiac risk prediction and restratification over and above current state-of-the-art assessment in coronary CTA by providing a quantitative measure of coronary inflammation. High perivascular FAI values (cutoff ≥-70·1 HU) are an indicator of increased cardiac mortality and, therefore, could guide early targeted primary prevention and intensive secondary prevention in patients.
Funding: British Heart Foundation, and the National Institute of Health Research Oxford Biomedical Research Centre.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Imaging of coronary inflammation for cardiovascular risk prediction.Lancet. 2018 Sep 15;392(10151):894-896. doi: 10.1016/S0140-6736(18)31716-1. Epub 2018 Aug 28. Lancet. 2018. PMID: 30170850 No abstract available.
-
Perivascular fat mapping predicts cardiac death.Nat Rev Cardiol. 2018 Nov;15(11):656. doi: 10.1038/s41569-018-0101-1. Nat Rev Cardiol. 2018. PMID: 30254256 No abstract available.
-
Detection of coronary inflammation.Lancet. 2019 Jun 1;393(10187):2198-2199. doi: 10.1016/S0140-6736(19)30225-9. Lancet. 2019. PMID: 31162077 No abstract available.
-
Detection of coronary inflammation.Lancet. 2019 Jun 1;393(10187):2198. doi: 10.1016/S0140-6736(19)30224-7. Lancet. 2019. PMID: 31162078 No abstract available.
References
-
- SCOT-HEART investigators CT coronary angiography in patients with suspected angina due to coronary heart disease (SCOT-HEART): an open-label, parallel-group, multicentre trial. Lancet. 2015;385:2383–2391. - PubMed
-
- The National Institute for Health and Care Excellence (NICE) Chest pain of recent onset: assessment and diagnosis. November, 2016. https://www.nice.org.uk/guidance/cg95 - PubMed
-
- Fishbein MC, Siegel RJ. How big are coronary atherosclerotic plaques that rupture? Circulation. 1996;94:2662–2666. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
