

High-sensitivity troponin in the evaluation of patients with suspected acute coronary syndrome: a stepped-wedge, cluster-randomised controlled trial
- PMID: 30170853
- PMCID: PMC6137538
- DOI: 10.1016/S0140-6736(18)31923-8
High-sensitivity troponin in the evaluation of patients with suspected acute coronary syndrome: a stepped-wedge, cluster-randomised controlled trial
Abstract
Background: High-sensitivity cardiac troponin assays permit use of lower thresholds for the diagnosis of myocardial infarction, but whether this improves clinical outcomes is unknown. We aimed to determine whether the introduction of a high-sensitivity cardiac troponin I (hs-cTnI) assay with a sex-specific 99th centile diagnostic threshold would reduce subsequent myocardial infarction or cardiovascular death in patients with suspected acute coronary syndrome.
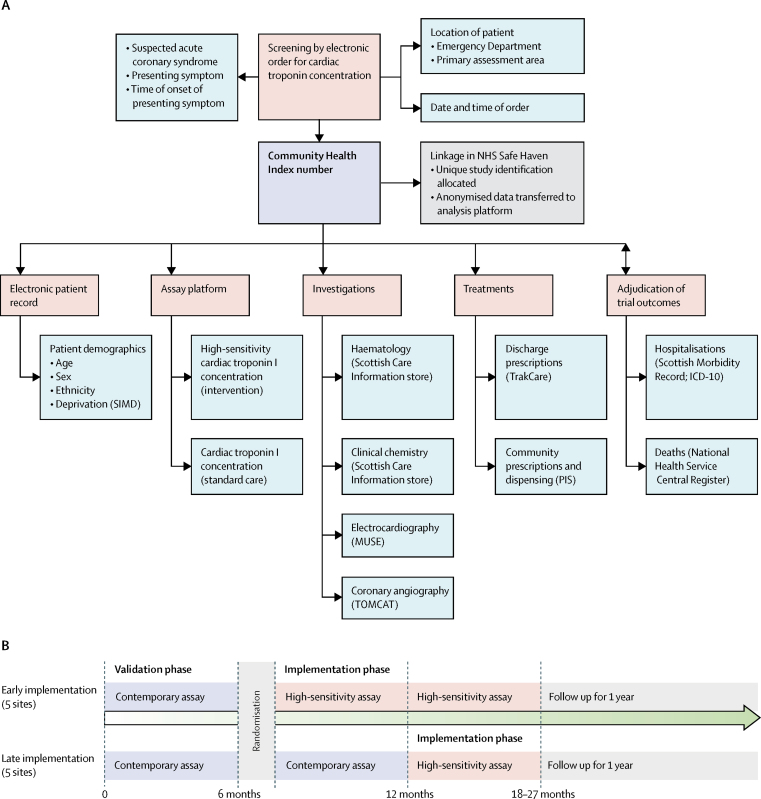
Methods: In this stepped-wedge, cluster-randomised controlled trial across ten secondary or tertiary care hospitals in Scotland, we evaluated the implementation of an hs-cTnI assay in consecutive patients who had been admitted to the hospitals' emergency departments with suspected acute coronary syndrome. Patients were eligible for inclusion if they presented with suspected acute coronary syndrome and had paired cardiac troponin measurements from the standard care and trial assays. During a validation phase of 6-12 months, results from the hs-cTnI assay were concealed from the attending clinician, and a contemporary cardiac troponin I (cTnI) assay was used to guide care. Hospitals were randomly allocated to early (n=5 hospitals) or late (n=5 hospitals) implementation, in which the high-sensitivity assay and sex-specific 99th centile diagnostic threshold was introduced immediately after the 6-month validation phase or was deferred for a further 6 months. Patients reclassified by the high-sensitivity assay were defined as those with an increased hs-cTnI concentration in whom cTnI concentrations were below the diagnostic threshold on the contemporary assay. The primary outcome was subsequent myocardial infarction or death from cardiovascular causes at 1 year after initial presentation. Outcomes were compared in patients reclassified by the high-sensitivity assay before and after its implementation by use of an adjusted generalised linear mixed model. This trial is registered with ClinicalTrials.gov, number NCT01852123.
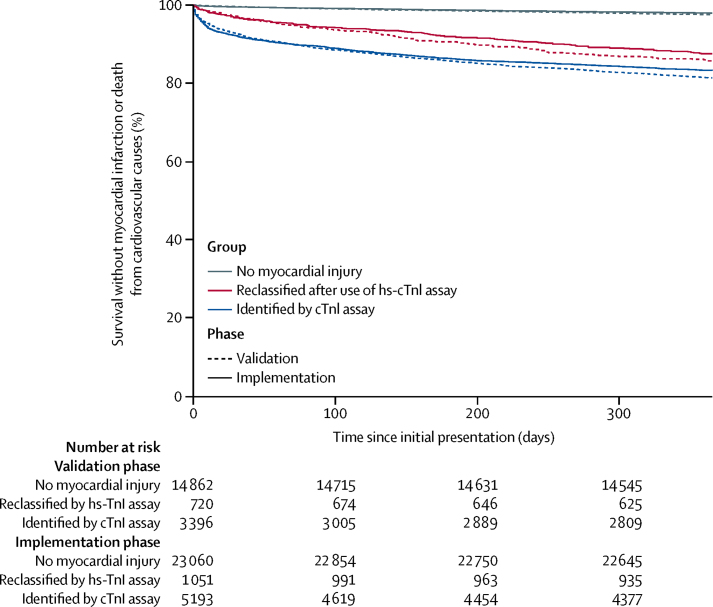
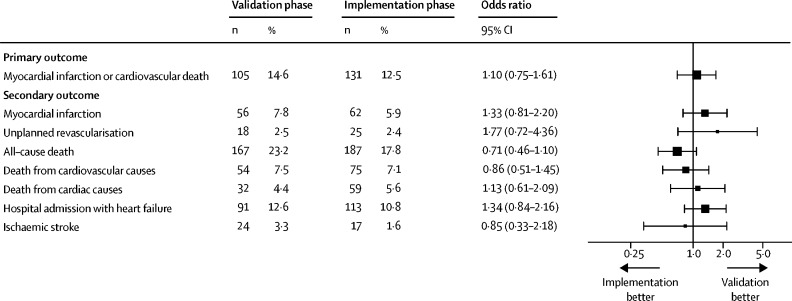
Findings: Between June 10, 2013, and March 3, 2016, we enrolled 48 282 consecutive patients (61 [SD 17] years, 47% women) of whom 10 360 (21%) patients had cTnI concentrations greater than those of the 99th centile of the normal range of values, who were identified by the contemporary assay or the high-sensitivity assay. The high-sensitivity assay reclassified 1771 (17%) of 10 360 patients with myocardial injury or infarction who were not identified by the contemporary assay. In those reclassified, subsequent myocardial infarction or cardiovascular death within 1 year occurred in 105 (15%) of 720 patients in the validation phase and 131 (12%) of 1051 patients in the implementation phase (adjusted odds ratio for implementation vs validation phase 1·10, 95% CI 0·75 to 1·61; p=0·620).
Interpretation: Use of a high-sensitivity assay prompted reclassification of 1771 (17%) of 10 360 patients with myocardial injury or infarction, but was not associated with a lower subsequent incidence of myocardial infarction or cardiovascular death at 1 year. Our findings question whether the diagnostic threshold for myocardial infarction should be based on the 99th centile derived from a normal reference population.
Funding: The British Heart Foundation.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Diagnosing myocardial infarction: a highly sensitive issue.Lancet. 2018 Sep 15;392(10151):893-894. doi: 10.1016/S0140-6736(18)31996-2. Epub 2018 Aug 28. Lancet. 2018. PMID: 30170849 No abstract available.
-
In suspected ACS, care based on high-sensitivity vs standard cardiac troponin I assays did not improve 1-y outcomes.Ann Intern Med. 2018 Dec 18;169(12):JC68. doi: 10.7326/ACPJC-2018-169-12-068. Ann Intern Med. 2018. PMID: 30557421 No abstract available.
References
-
- Thygesen K, Alpert JS, Jaffe AS. Third universal definition of myocardial infarction. Circulation. 2012;126:2020–2035. - PubMed
-
- Apple FS, Collinson PO. Analytical characteristics of high–sensitivity cardiac troponin assays. Clin Chem. 2012;58:54–61. - PubMed
-
- Kimenai DM, Janssen EBNJ, Eggers KM. Sex-specific versus overall clinical decision limits for cardiac troponin I and T for the diagnosis of acute myocardial infarction: a systematic review. Clin Chem. 2018;64:1034–1043. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
