

Clinical and molecular characteristics of MEF2D fusion-positive B-cell precursor acute lymphoblastic leukemia in childhood, including a novel translocation resulting in MEF2D-HNRNPH1 gene fusion
- PMID: 30171027
- PMCID: PMC6312004
- DOI: 10.3324/haematol.2017.186320
Clinical and molecular characteristics of MEF2D fusion-positive B-cell precursor acute lymphoblastic leukemia in childhood, including a novel translocation resulting in MEF2D-HNRNPH1 gene fusion
Abstract
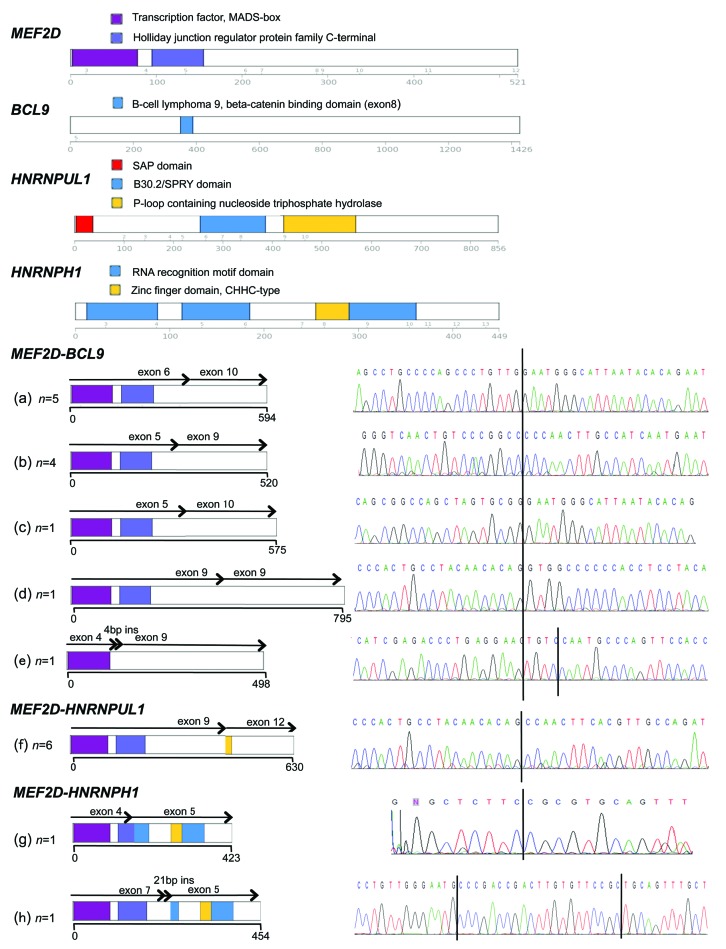
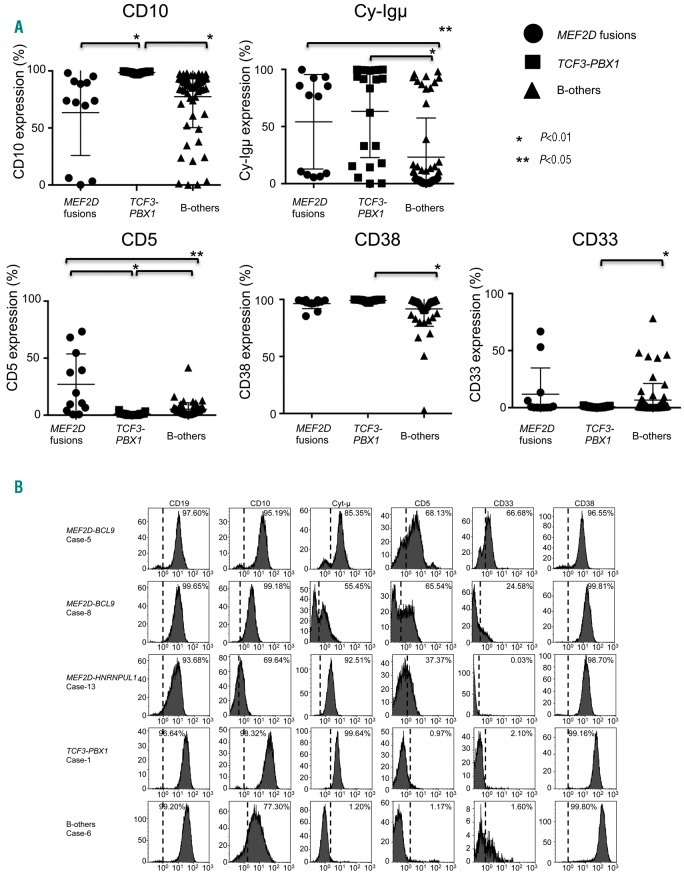
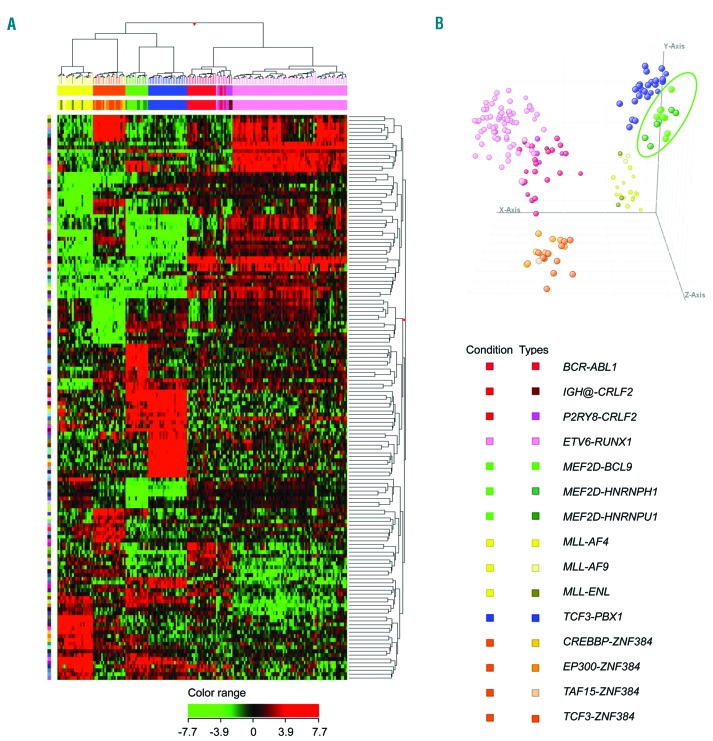
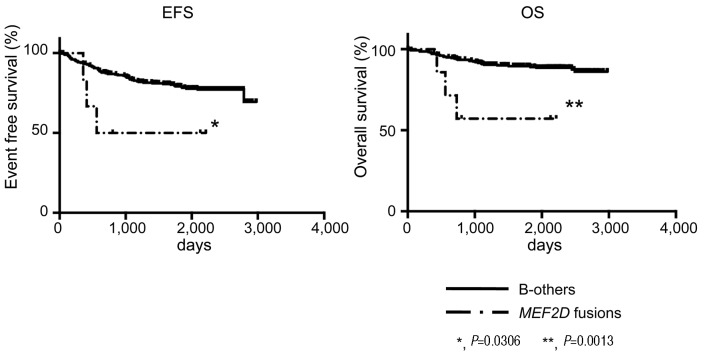
Fusion genes involving MEF2D have recently been identified in precursor B-cell acute lymphoblastic leukemia, mutually exclusive of the common risk stratifying genetic abnormalities, although their true incidence and associated clinical characteristics remain unknown. We identified 16 cases of acute lymphoblastic leukemia and 1 of lymphoma harboring MEF2D fusions, including MEF2D-BCL9 (n=10), MEF2D-HNRNPUL1 (n=6), and one novel MEF2D-HNRNPH1 fusion. The incidence of MEF2D fusions overall was 2.4% among consecutive precursor B-cell acute lymphoblastic leukemia patients enrolled onto a single clinical trial. They frequently showed a cytoplasmic μ chain-positive pre-B immunophenotype, and often expressed an aberrant CD5 antigen. Besides up- and down-regulation of HDAC9 and MEF2C, elevated GATA3 expression was also a characteristic feature of MEF2D fusion-positive patients. Mutations of PHF6, recurrent in T-cell acute lymphoblastic leukemia, also showed an unexpectedly high frequency (50%) in these patients. MEF2D fusion-positive patients were older (median age 9 years) with elevated WBC counts (median: 27,300/ml) at presentation and, as a result, were mostly classified as NCI high risk. Although they responded well to steroid treatment, MEF2D fusion-positive patients showed a significantly worse outcome, with 53.3% relapse and subsequent death. Stem cell transplantation was ineffective as salvage therapy. Interestingly, relapse was frequently associated with the presence of CDKN2A/CDKN2B gene deletions. Our observations indicate that MEF2D fusions comprise a distinct subgroup of precursor B-cell acute lymphoblastic leukemia with a characteristic immunophenotype and gene expression signature, associated with distinct clinical features.
Copyright© 2019 Ferrata Storti Foundation.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
