

Evaluation of atrial septal defects with 4D flow MRI-multilevel and inter-reader reproducibility for quantification of shunt severity
- PMID: 30171383
- PMCID: PMC6424937
- DOI: 10.1007/s10334-018-0702-z
Evaluation of atrial septal defects with 4D flow MRI-multilevel and inter-reader reproducibility for quantification of shunt severity
Abstract
Purpose: With the hypothesis that 4D flow can be used in evaluation of cardiac shunts, we seek to evaluate the multilevel and interreader reproducibility of measurements of the blood flow, shunt fraction and shunt volume in patients with atrial septum defect (ASD) in practice at multiple clinical sites.
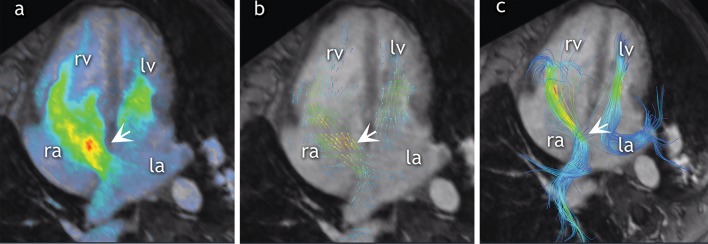
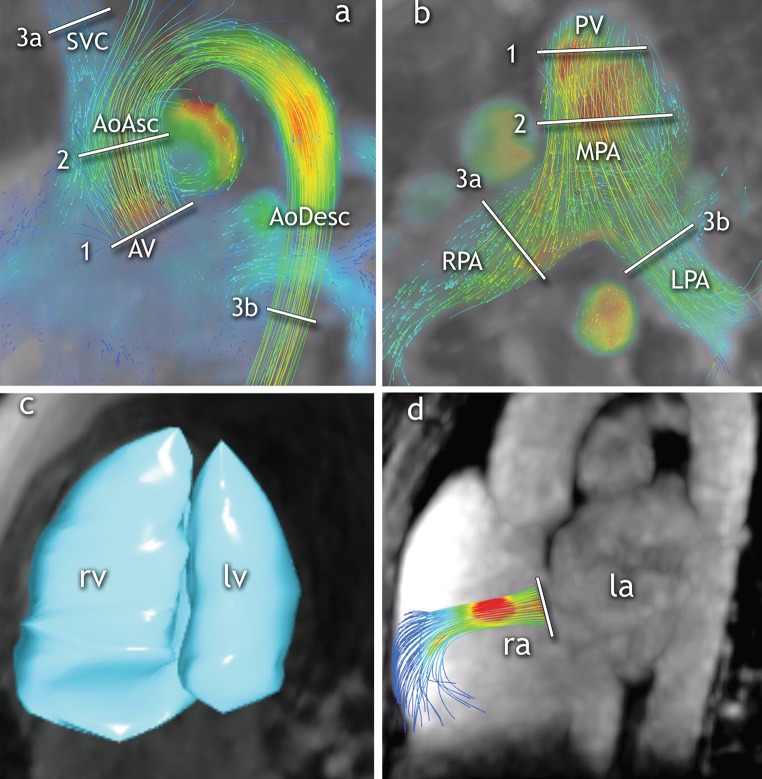
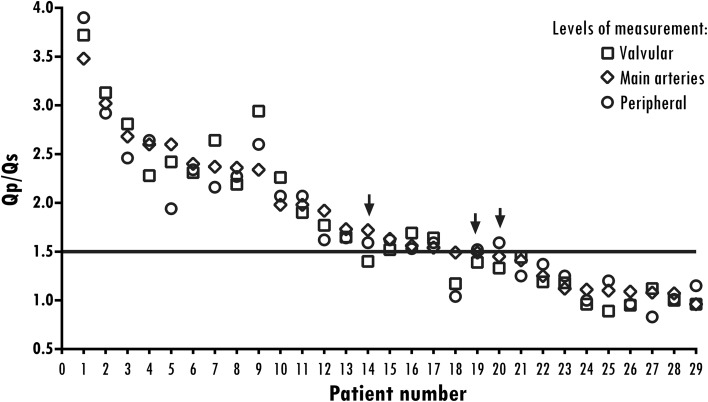
Materials and methods: Four-dimensional flow MRI examinations were performed at four institutions across Europe and the US. Twenty-nine patients (mean age, 43 years; 11 male) were included in the study. Flow measurements were performed at three levels (valve, main artery and periphery) in both the pulmonary and systemic circulation by two independent readers and compared against stroke volumes from 4D flow anatomic data. Further, the shunt ratio (Qp/Qs) was calculated. Additionally, shunt volume was quantified at the atrial level by tracking the atrial septum.
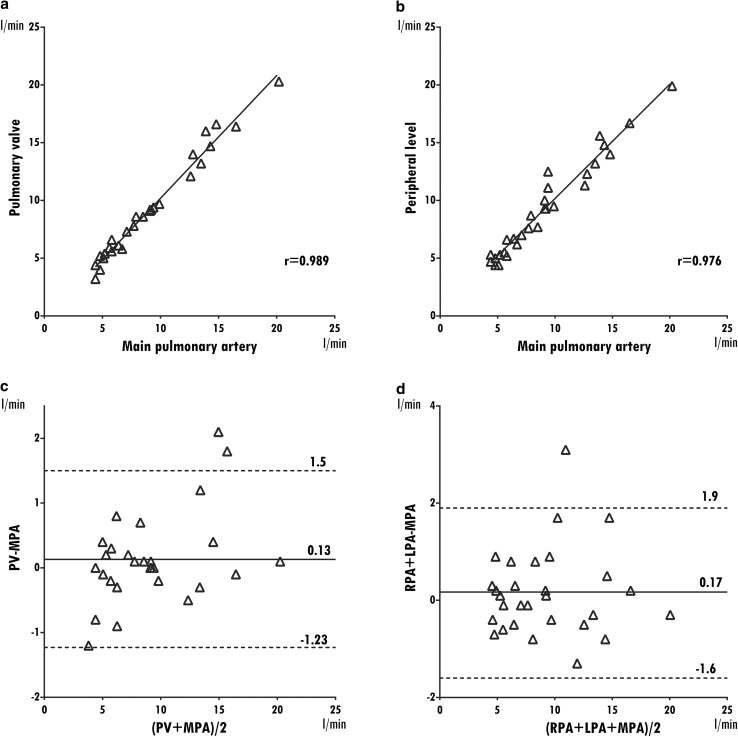
Results: Measurements of the pulmonary blood flow at multiple levels correlate well whether measuring at the valve, main pulmonary artery or branch pulmonary arteries (r = 0.885-0.886). Measurements of the systemic blood flow show excellent correlation, whether measuring at the valve, ascending aorta or sum of flow from the superior vena cava (SVC) and descending aorta (r = 0.974-0.991). Intraclass agreement between the two observers for the flow measurements varies between 0.96 and 0.99. Compared with stroke volume, pulmonic flow is underestimated with 0.26 l/min at the main pulmonary artery level, and systemic flow is overestimated with 0.16 l/min at the ascending aorta level. Direct measurements of ASD flow are feasible in 20 of 29 (69%) patients.
Conclusion: Blood flow and shunt quantification measured at multiple levels and performed by different readers are reproducible and consistent with 4D flow MRI.
Keywords: 4D flow MRI; Atrial septal defect; Multiple measurements.
Conflict of interest statement
Conflict of interest
R.G. Chelu received funding for research from GE Healthcare and is a consultant to Arterys, Inc. J.W. Roos-Hesellink received a grant from the Dutch Heart Foundation. K. Nieman reports non-financial support from Siemens Medical Solutions and grants from GE Healthcare and Bayer Healthcare, outside the submitted work. S.S. Vasanawala is involved in research collaboration with GE Healthcare, is founder of and consultant to Arterys, Inc., and received a research grant from Bayer AG. A. Hsiao is founder of and consultant to Arterys, Inc., and received a research grant from GE Healthcare. The rest of the authors report no conflict of interest.
Ethical standards
Patient studies were aggregated from multiple centers and approved by each local IRB, including either a waiver of consent or prospective enrollment with signed consent, as deemed appropriate by each center. The study protocol was compliant with the Declaration of Helsinki.
Figures

References
-
- Roos-Hesselink JW, Meijboom FJ, Spitaels SEC et al (2003) Excellent survival and low incidence of arrhythmias, stroke and heart failure long-term after surgical ASD closure at young age. A prospective follow-up study of 21–33 years. Eur Heart J 24(2):190–197. http://www.ncbi.nlm.nih.gov/pubmed/12573276. Accessed Feb 27 2017 - PubMed
-
- Cuypers JAAE, Opić P, Menting ME et al (2013) The unnatural history of an atrial septal defect: longitudinal 35 year follow up after surgical closure at young age. Heart BMJ Publ Group Ltd British Cardiovascular Soc 99(18):1346–1352. http://www.ncbi.nlm.nih.gov/pubmed/23886606. Accessed Feb 24 2017 - PubMed
-
- Warnes CA, Williams RG, Bashore TM et al (2008) ACC/AHA 2008 Guidelines for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (writing committee to develop guidelines on the management of a. Circulation 118(23):e714–e833. http://www.ncbi.nlm.nih.gov/pubmed/18997169. Accessed December 2, 2014 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
