

Could Intensive Blood Pressure Control Really Reduce Diabetic Retinopathy Outcomes? Evidence from Meta-Analysis and Trial Sequential Analysis from Randomized Controlled Trials
- PMID: 30171589
- PMCID: PMC6167290
- DOI: 10.1007/s13300-018-0497-y
Could Intensive Blood Pressure Control Really Reduce Diabetic Retinopathy Outcomes? Evidence from Meta-Analysis and Trial Sequential Analysis from Randomized Controlled Trials
Retraction in
-
Retraction Note: Could Intensive Blood Pressure Control Really Reduce Diabetic Retinopathy Outcomes? Evidence from Meta-Analysis and Trial Sequential Analysis from Randomized Controlled Trials.Diabetes Ther. 2023 May;14(5):951. doi: 10.1007/s13300-023-01396-3. Diabetes Ther. 2023. PMID: 36932297 Free PMC article. No abstract available.
Abstract
Introduction: To explore the accumulated evidence concerning the effect of intensive blood pressure control on the incidence and progression of diabetic retinopathy (DR), proliferative diabetic retinopathy (PDR) and macular edema (ME).
Methods: A number of electronic databases were searched including PubMed, EMBASE, CINAHL, Cochrane Library, conferences and proceedings. Randomized controlled trials comparing intensive blood pressure targets with conventional blood pressure targets in patients with type 2 diabetes were included. The definition of intensive versus conventional blood pressure targets was from the pertinent original studies. Meta-analyses and trial sequential analyses of randomized trials were analyzed in STATA.
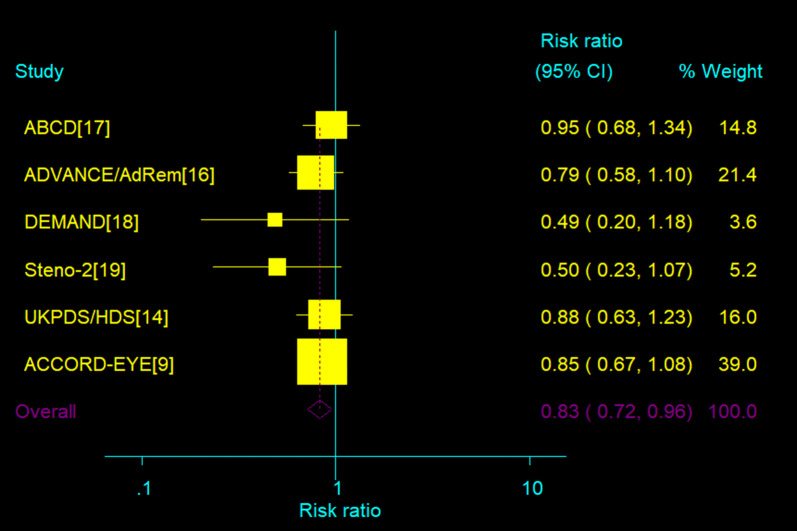
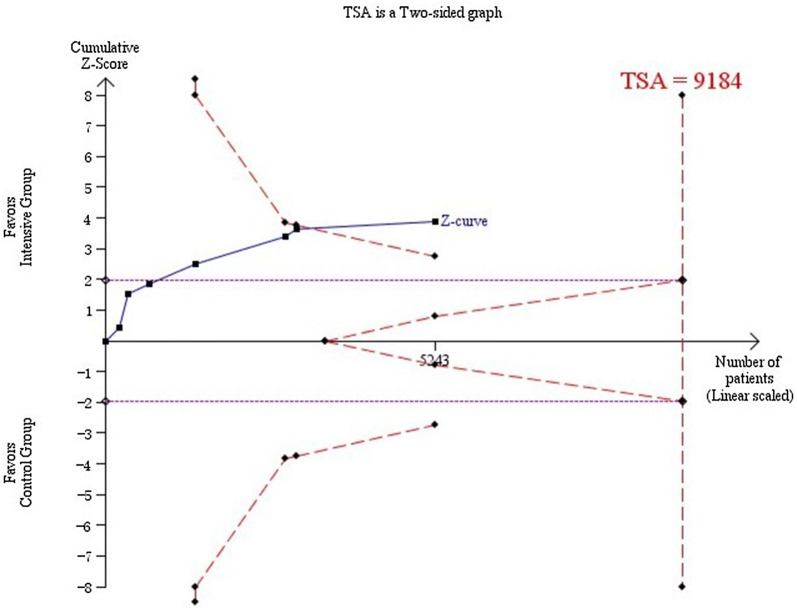
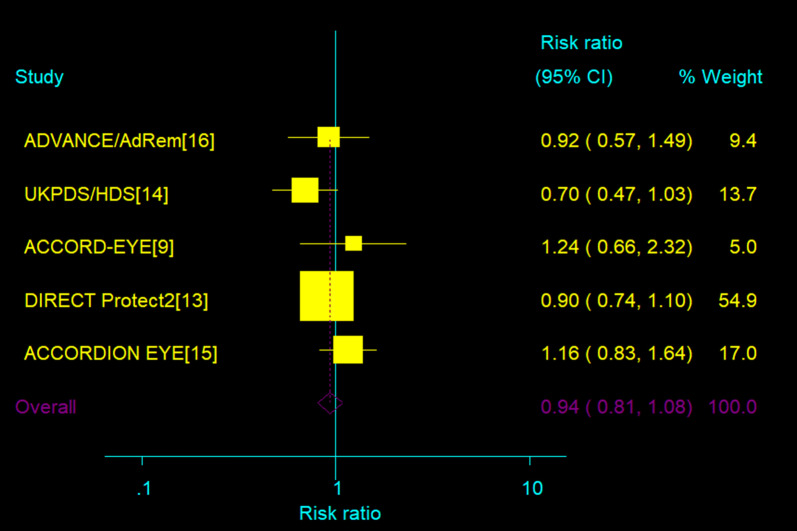
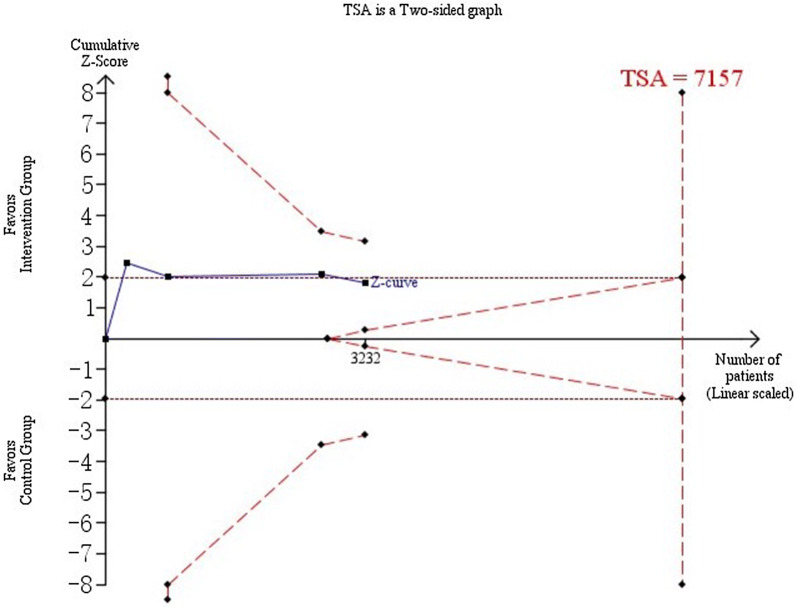
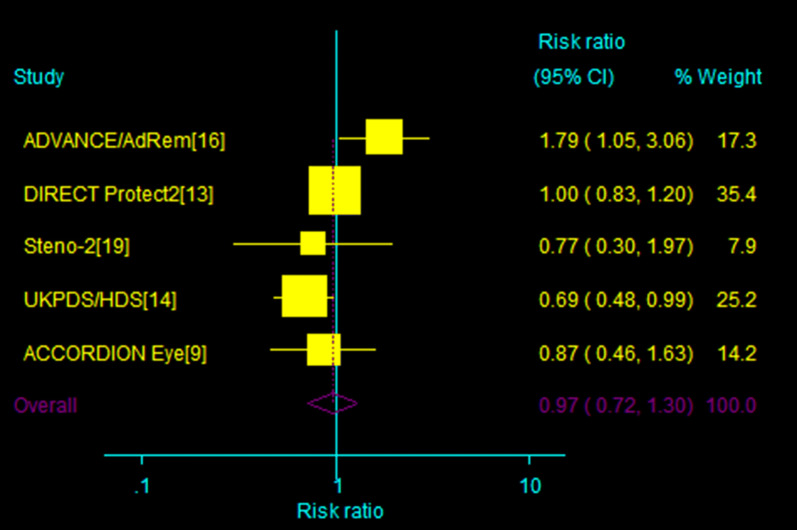
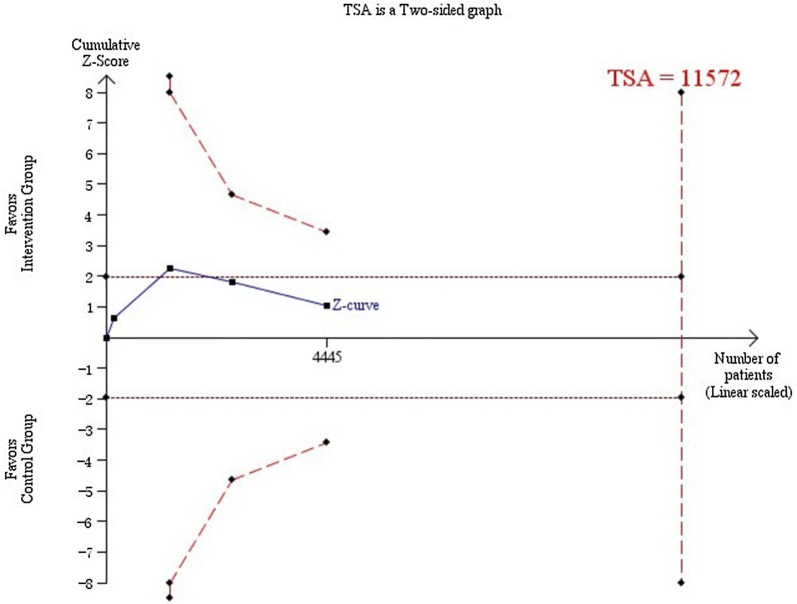
Results: Eight trials randomizing 6989 patients were assessed and reviewed in full text; 3749 vs. 3240 were in each arm (intensive vs. conventional). All trials had a low risk of bias. Intensive blood pressure control supported a 17% reduction in the incidence of DR (relative risk 0.83, 95% confidence interval 0.72-0.95). Trial sequential analyses confirmed that sufficient evidence indicated a relative risk reduction above 17% for the incidence of DR when intensive blood pressure control was targeted. Heterogeneity was absent (I2 = 0%; P = 0.56). No statistically significant effect was found for intensive blood pressure targeting on the progress of DR (relative risk 0.94, 95% confidence interval 0.81-1.08). TSA showed that insufficient evidence had been found, although the Z value line appeared to have a tendency of approaching the futility boundaries. There were also no statistically significant effects on the incidence of PDR and ME (TSA-adjusted CI 0.84-1.12).
Conclusion: Intensive blood pressure control reduced the relative risk of incidence of DR by 17%. The available data were insufficient to prove or refute a relative risk reduction for the progression of DR or incidence of PDR and ME at a magnitude of 15%.
Keywords: Diabetic retinopathy; Intensive blood pressure control; Trial sequential analysis.
Conflict of interest statement
The authors, Jian-Bo Zhou, Zhi-Hui Song, Lu Bai, Xiao-Rong Zhu, Hong-Bing Li and Jin-Kui Yang, have nothing to disclose.
Figures
References
-
- Malek M, Khamseh ME, Aghili R, Emami Z, Najafi L, Baradaran HR. Medical management of diabetic retinopathy: an overview. Arch Iran Med. 2012;15(10):635–640. - PubMed
-
- Ohashi K, Hayashi T, Watanabe Y, Hara K, Ukichi R, Asano H, Suzuki H, Yamashiro K, Tojo K, Sakamoto M, Utsunomiya K. Primary aldosteronism with type 2 diabetes mellitus requires more antihypertensive drugs for blood pressure control: a retrospective observational study. J Clin Med Res. 2018;10(1):56–62. doi: 10.14740/jocmr3233w. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
