

Living-related kidney transplantation with catheterizable urinary conduit in prune belly syndrome: A case report
- PMID: 30172052
- PMCID: PMC6122431
- DOI: 10.1016/j.ijscr.2018.08.022
Living-related kidney transplantation with catheterizable urinary conduit in prune belly syndrome: A case report
Abstract
Introduction: Prune belly syndrome (PBS) presents with both renal dysplasia and urinary tract abnormalities. When performing kidney transplantation in PBS patients with kidney failure, extensive pretransplant urinary tract preparation may be necessary.
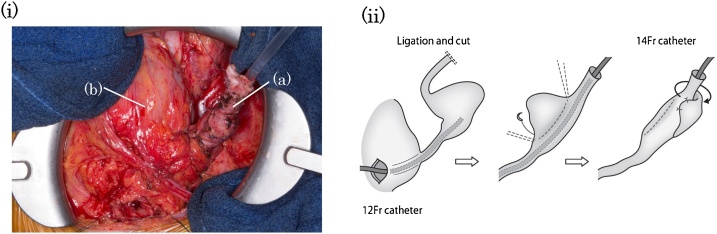
Presentation of case: We report the case of a 36-year-old man with PBS who underwent living-related kidney transplantation with urinary diversion using the Mitrofanoff principle. The patient had a bilateral loop ureterostomy for a urethral obstruction. Cystourethrography before the operation showed tortuous and dilated ureters with vesicoureteral reflux (VUR), and complete occlusion of the urethra. Before transplantation, we created a catheterizable urinary conduit with the patient's own malformed left ureter in accordance with the Mitrofanoff principle. The folding procedure was selected for ureteroplasty to preserve good blood supply. Extravesical detrusorrhaphy was performed as an antireflux procedure. V-quadrilateral-Z ureterostomy for catheterization was performed. Then, we performed living-related kidney transplantation from the patient's mother. Postoperative cystourethrography did not show left VUR. The patient performed clean intermittent self-catheterization without complications, and had good graft function.
Discussion: The appendix and ileum are currently the most commonly used options for urinary conduits based on the Mitrofanoff principle. However, the patient had complications of diarrhoea and constipation, so we used the patient's own malformed ureter. We performed a folding procedure to avoid ureteral stenosis and VUR, and used the V-quadrilateral-Z flap technique to avoid stoma stenosis CONCLUSION: When performing kidney transplantation in patients with PBS, urinary tract anomalies should be thoroughly evaluated. Our surgical procedure will help to reduce complications after kidney transplantation.
Keywords: Kidney transplantation; Mitrofanoff principle; Prune belly syndrome; Urinary diversion.
Copyright © 2018 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures


References
-
- Reinberg Y., Manivel J.C., Pettinato G., Gonzalez R. Development of renal failure in children with the prune belly syndrome. J. Urol. 1991;145:1017–1019. - PubMed
-
- Routh J.C., Huang L., Retik A.B., Nelson C.P. Contemporary epidemiology and characterization of newborn males with prune belly syndrome. Urology. 2010;76:44–48. - PubMed
-
- Kamel M.H., Thomas A.A., Al-Mufarrej F.M., O’Kelly P., Hickey D.P. Deceased-donor kidney transplantation in prune belly syndrome. Urology. 2007;69:666–669. - PubMed
-
- Djakovic N., Wagener N., Adams J., Gilfrich C., Haferkamp A., Pfitzenmaier J. Intestinal reconstruction of the lower urinary tract as a prerequisite for renal transplantation. BJU Int. 2009;103:1555–1560. - PubMed
-
- Agha R.A., Fowler A.J., Saeta A., Barai I., Rajmohan S., Orgill D.P. Erratum to "The SCARE guidelines: consensus-based surgical case report guidelines" [Int. J. Surg. 34 (2016) 180-186] Int. J. Surg. 2016;36(Pt A):396. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
