

Pediatric lung adenocarcinoma presenting with brain metastasis: a case report
- PMID: 30172261
- PMCID: PMC6119591
- DOI: 10.1186/s13256-018-1781-1
Pediatric lung adenocarcinoma presenting with brain metastasis: a case report
Abstract
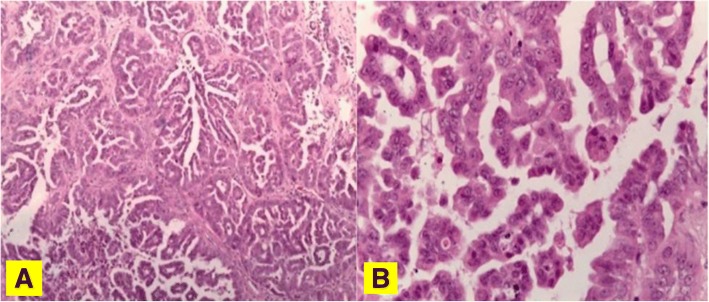
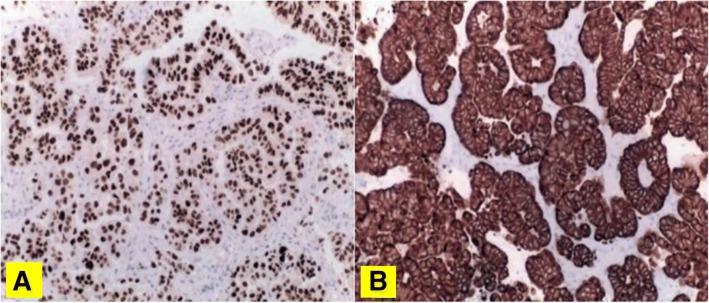
Background: Diagnosis and treatment of primary lung adenocarcinoma in children remains challenging given its rarity. Here we highlight the clinical history, pathological evaluation, genomic findings, and management of a very young patient with metastatic lung adenocarcinoma.
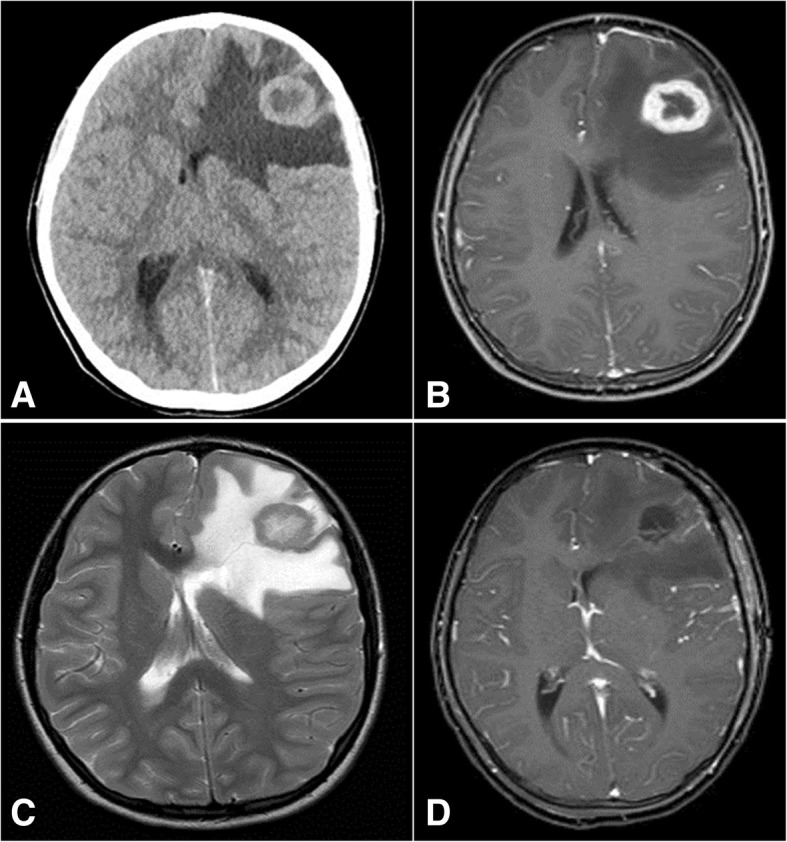
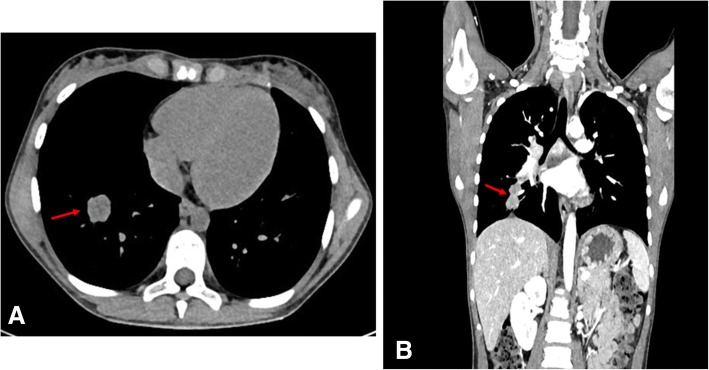
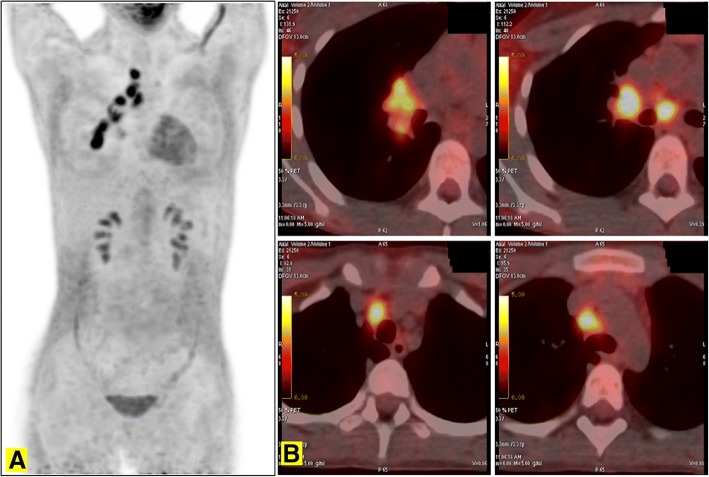
Case presentation: A 10-year-old white girl presented with brain metastases due to primary pulmonary adenocarcinoma. Next generation sequencing analysis with "Comprehensive Cancer Panel" highlighted the presence of multiple non-targetable mutations in the FLT4, UBR5, ATM, TAF1, and GUCY1A2 genes. She was treated aggressively with chemotherapy, surgery, and radiation therapy for local and distant recurrence. Eventually, therapy with nivolumab was started compassionately, and she died 23 months after diagnosis.
Conclusions: Extremely rare cancers in children such as lung adenocarcinoma need accurate and specific diagnosis in order to develop an optimal plan of treatment. It is also necessary to underline that "children are not little adults," thus implying that an adult-type cancer in the pediatric population might have a different etiopathogenesis. Diagnostic confirmation and primary treatment of such rare conditions should be centralized in reference centers, collaborative networks, or both, with multidisciplinary approaches and very specific expertise.
Keywords: Brain metastasis; Cancer immunotherapy; Lung adenocarcinoma; Nivolumab; Rare tumor; TREP.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the institutional review board at the AORN Santobono-Pausilipon, Naples.
Consent for publication
Written informed consent was obtained from the patient’s legal guardian(s) for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
