

Practice Pattern Variation in the Use of Transesophageal Echocardiography for Open Valve Cardiac Surgery
- PMID: 30174265
- PMCID: PMC6310636
- DOI: 10.1053/j.jvca.2018.07.040
Practice Pattern Variation in the Use of Transesophageal Echocardiography for Open Valve Cardiac Surgery
Abstract
Objective: The authors sought to assess for the presence of practice variation in the use of intraoperative transesophageal echocardiography (TEE) for open cardiac valve surgery.
Design: This study was a retrospective cohort analysis.
Setting: The administrative claims data used for this investigation were multi-institutional and a representative sample of commercially insured patients in the United States between 2010 and 2015.
Participants: The cohort consisted of adult patients, aged 18 years or older, undergoing open mitral valve (MV) or aortic valve (AV) surgery.
Interventions: This was an observational analysis without interventions.
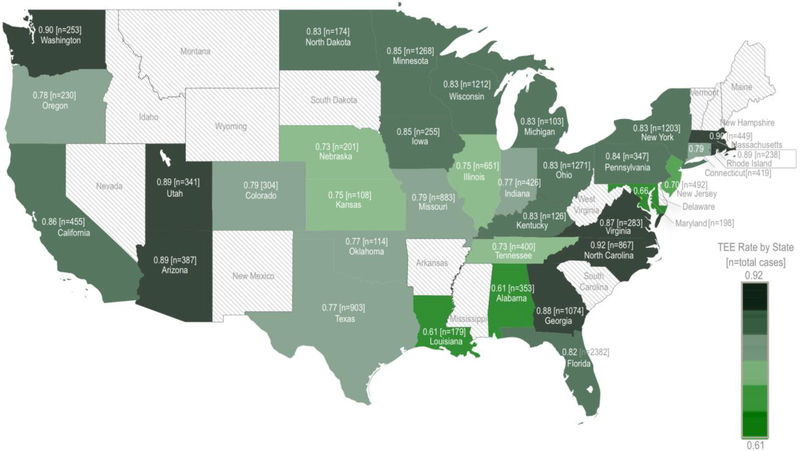
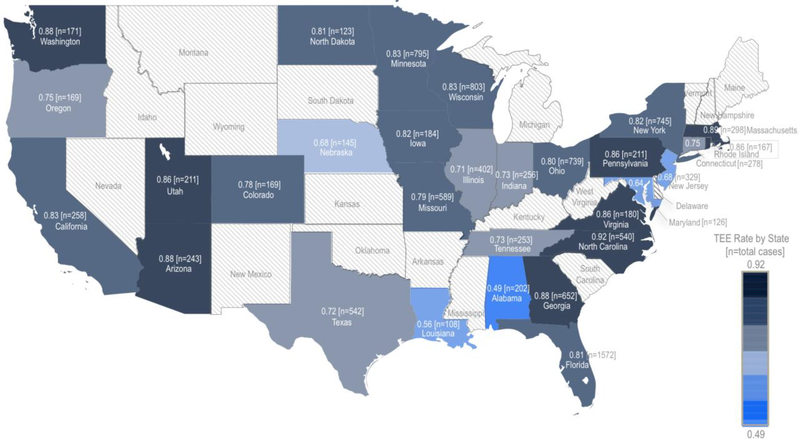
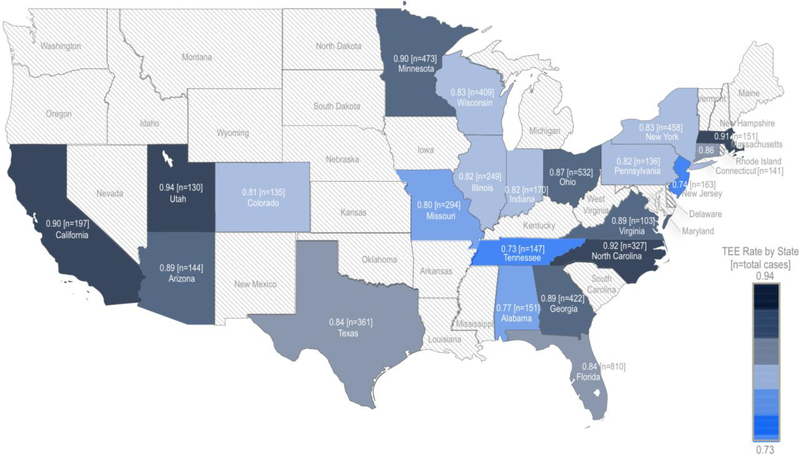
Measurements and main results: Of 19,386 valve surgeries, 12,313 (64%) underwent AV replacement, 6,192 (32%) underwent MV repair or replacement, and 881 (<5%) underwent both MV and AV surgery. The overall rate of intraoperative TEE was 82% (95% confidence interval [CI]: 81%-82%), less frequently observed in AV procedures compared to MV or combined MV-AV procedures (80% v 85%, p < 0.001). Rates of intraoperative TEE claims varied markedly across U.S. states. After adjustment, the relative odds of an intraoperative TEE claim ranged across states from 0.26 (Louisiana, 95% CI: 0.18-0.36; p < 0.001) to 2.10 (North Carolina, 95% CI: 1.57-2.82; p < 0.001).
Conclusion: Among adult patients undergoing open AV or MV surgery in the United States, 82% had a claim for an intraoperative TEE with marked variability across U.S. states. Increasing adherence to intraoperative TEE guidelines for valve surgery may represent an unrecognized opportunity to improve the quality of cardiac surgical care.
Keywords: aortic valve surgery; cardiovascular surgery; ethics and policy; guideline compliance and adherence; health services; intraoperative echocardiography; mitral valve surgery; transesophageal echocardiography.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest:
All co-authors declare no competing interests
Figures
Comment in
-
Practice Patterns for the Use of Perioperative Transesophageal Echocardiography: A Practice not yet Made Perfect.J Cardiothorac Vasc Anesth. 2019 Jan;33(1):134-136. doi: 10.1053/j.jvca.2018.09.004. Epub 2018 Sep 12. J Cardiothorac Vasc Anesth. 2019. PMID: 30293830 No abstract available.
Similar articles
-
Association of Intraoperative Transesophageal Echocardiography and Clinical Outcomes After Open Cardiac Valve or Proximal Aortic Surgery.JAMA Netw Open. 2022 Feb 1;5(2):e2147820. doi: 10.1001/jamanetworkopen.2021.47820. JAMA Netw Open. 2022. PMID: 35138396 Free PMC article.
-
Transesophageal Echocardiography, Mortality, and Length of Hospitalization after Cardiac Valve Surgery.J Am Soc Echocardiogr. 2020 Jun;33(6):756-762.e1. doi: 10.1016/j.echo.2020.01.014. Epub 2020 Mar 26. J Am Soc Echocardiogr. 2020. PMID: 32222480 Free PMC article.
-
Assessment of Paravalvular Leak After Transcatheter Aortic Valve Replacement: Transesophageal Echocardiography Compared With Transthoracic Echocardiography.J Cardiothorac Vasc Anesth. 2017 Aug;31(4):1278-1284. doi: 10.1053/j.jvca.2017.03.010. Epub 2017 Mar 7. J Cardiothorac Vasc Anesth. 2017. PMID: 28800985
-
The role of intraoperative echocardiography in valve surgery.Cardiol Clin. 1998 Aug;16(3):477-89, ix. doi: 10.1016/s0733-8651(05)70027-8. Cardiol Clin. 1998. PMID: 9742326 Review.
-
Transesophageal echocardiography and adult cardiac operations.Ann Thorac Surg. 1995 Mar;59(3):773-9. doi: 10.1016/0003-4975(94)00818-3. Ann Thorac Surg. 1995. PMID: 7887737 Review.
Cited by
-
Patient-, Clinician-, and Institution-level Variation in Inotrope Use for Cardiac Surgery: A Multicenter Observational Analysis.Anesthesiology. 2023 Aug 1;139(2):122-141. doi: 10.1097/ALN.0000000000004593. Anesthesiology. 2023. PMID: 37094103 Free PMC article.
-
Testing clinical selection criteria for intraoperative transoesophageal echocardiography in isolated coronary artery bypass graft surgery.BJA Open. 2024 Mar 22;10:100278. doi: 10.1016/j.bjao.2024.100278. eCollection 2024 Jun. BJA Open. 2024. PMID: 38550531 Free PMC article.
-
Accounting for Healthcare Structures When Measuring Variation in Care.Anesthesiology. 2025 May 1;142(5):793-805. doi: 10.1097/ALN.0000000000005395. Epub 2025 Apr 8. Anesthesiology. 2025. PMID: 40197451 Review.
-
Transesophageal Echocardiography in Patients Undergoing Coronary Artery Bypass Graft Surgery.J Am Coll Cardiol. 2021 Jul 13;78(2):112-122. doi: 10.1016/j.jacc.2021.04.064. Epub 2021 May 3. J Am Coll Cardiol. 2021. PMID: 33957241 Free PMC article.
-
Multicentre analysis of practice patterns regarding benzodiazepine use in cardiac surgery.Br J Anaesth. 2022 May;128(5):772-784. doi: 10.1016/j.bja.2021.11.040. Epub 2022 Jan 29. Br J Anaesth. 2022. PMID: 35101244 Free PMC article.
References
-
- Nkomo VT, Gardin JM, Skelton TN, et al.: Burden of valvular heart diseases: a population-based study. Lancet. 368:1005–1011, 2006. - PubMed
-
- Surgeons ESSoT: Executive Summary Adult Cardiac Surgery Database. vol 2016. Society of Thoracic Surgeons; 2015.
-
- American Society of A, Society of Cardiovascular Anesthesiologists Task Force on Transesophageal E: Practice guidelines for perioperative transesophageal echocardiography. An updated report by the American Society of Anesthesiologists and the Society of Cardiovascular Anesthesiologists Task Force on Transesophageal Echocardiography. Anesthesiology. 112:1084–1096, 2010. - PubMed
-
- American College of Cardiology Foundation Appropriate Use Criteria Task F, American Society of E, American Heart A, et al.: ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 Appropriate Use Criteria for Echocardiography. A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Society of Echocardiography, American Heart Association, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Critical Care Medicine, Society of Cardiovascular Computed Tomography, and Society for Cardiovascular Magnetic Resonance Endorsed by the American College of Chest Physicians. J Am Coll Cardiol. 57:1126–1166, 2011. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, et al.: 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Thorac Cardiovasc Surg. 148:e1–e132, 2014. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
