

Independent factors related to preoperative acute lung injury in 130 adults undergoing Stanford type-A acute aortic dissection surgery: a single-center cross-sectional clinical study
- PMID: 30174890
- PMCID: PMC6105969
- DOI: 10.21037/jtd.2018.06.140
Independent factors related to preoperative acute lung injury in 130 adults undergoing Stanford type-A acute aortic dissection surgery: a single-center cross-sectional clinical study
Abstract
Background: Previous retrospective study suggested that acute lung injury (ALI) is frequent (78.49%) in patients undergoing aortic dissection surgery, and accompanied by a number of untoward consequences, and even induces death.
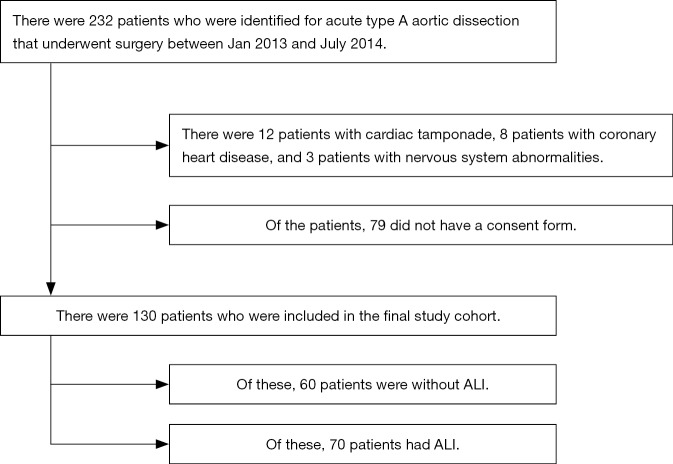
Methods: This prospective single-center cross-sectional study, registered in the ClinicalTrials.gov (Identifier: NCT01894334), assessed the preoperative clinical variables and serological results from 130 adult patients scheduled for Stanford type-A acute aortic dissection (AAD) surgery at Beijing Anzhen Hospital between January 2013 and July 2014. Exclusion criteria included patients with coronary heart disease, severe heart failure, severe cardiac tamponade and severe nervous system abnormalities. Preoperative ALI was identified according to oxygenation index (OI) calculated by PaO2/FiO2 ratio after anesthesia induction, and all the patients were divided into two groups: non-ALI (OI ≥300 mmHg) and ALI (OI <300 mmHg). The primary endpoint was the incidence of preoperative ALI. The secondary endpoints were the independent factors affecting the occurrence of preoperative ALI.
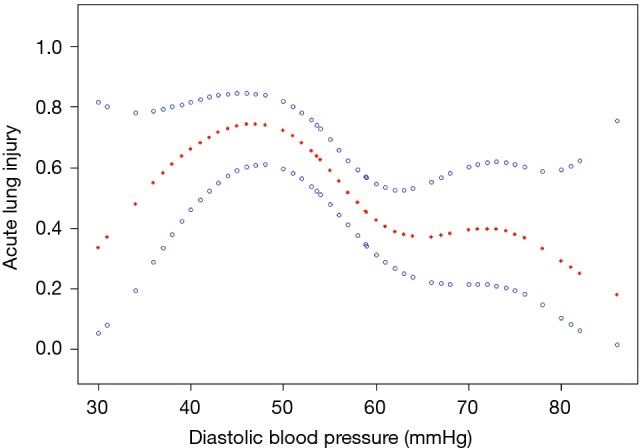
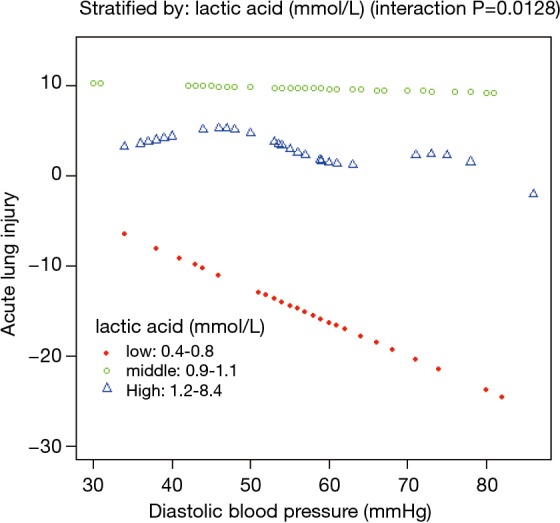
Results: The incidence of preoperative ALI was 53.8%. With adjusted multiple logistic regression analysis, age [odds ratio (OR) 1.14, confidence interval (CI), 1.06-1.22; P=0.0002], body mass index (BMI) (OR 1.31, CI, 1.09-1.56; P=0.0033), preoperative diastolic blood pressure (DBP) (OR 0.94, CI, 0.89-0.99; P=0.0109), interleukin-6 (IL-6) (OR 1.03, 95% CI, 1.01-1.06; P=0.0053), and prostaglandin I2/thromboxane B2 (PGI2/TXB2) ratio (OR 0.25, 95% CI, 0.09-0.67; P=0.0055) were significantly related to the occurrence of preoperative ALI. The decreased risk of ALI was related to the preoperative DBP value up to 44 mmHg (OR 0.935, 95% CI, 0.895-0.978; P=0.0033). Interactions analysis revealed that serum lactic acid mediated the relationship between DBP and ALI before Stanford type-A AAD surgery.
Conclusions: In adults undergoing Stanford type-A AAD surgery, the incidence of preoperative ALI was 53.8%, and age, BMI, preoperative DBP, IL-6, and PGI2/TXB2 ratio were independent factors related to the occurrence of pre-operative ALI. Trial Registration: ClinicalTrials.gov, Identifier: NCT01894334.
Keywords: Acute lung injury (ALI); Stanford type-A acute aortic dissection surgery; cross-sectional study.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Hasegawa Y, Ishikawa S, Ohtaki A, et al. Impaired lung oxygenation in acute aortic dissection. J Cardiovasc Surg (Torino) 1999;40:191-5. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical