

Moderate Aortic Stenosis and Reduced Left Ventricular Ejection Fraction: Current Evidence and Challenges Ahead
- PMID: 30175103
- PMCID: PMC6107690
- DOI: 10.3389/fcvm.2018.00111
Moderate Aortic Stenosis and Reduced Left Ventricular Ejection Fraction: Current Evidence and Challenges Ahead
Abstract
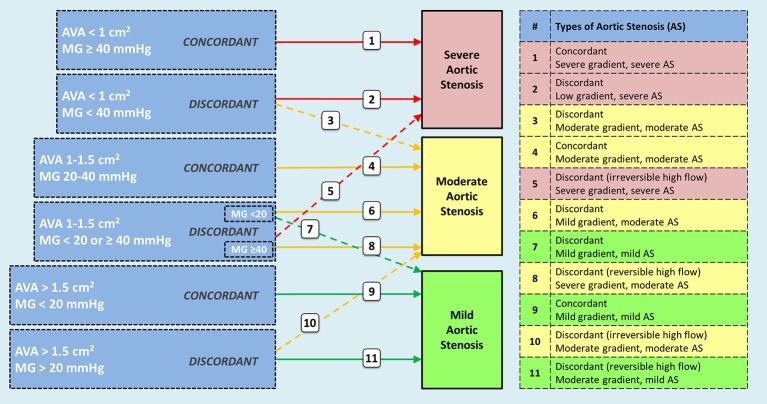
Moderate aortic stenosis (AS) and reduced left ventricular ejection fraction (LVEF) constitute a clinical entity that has been proposed as a therapeutic target for transcatheter aortic valve replacement (TAVR). It is defined by a mean trans-aortic gradient between 20 and 40 mmHg and an aortic valve area between 1.0 and 1.5 cm2 in patients with LVEF < 50%. Retrospective data suggests a prevalence of 0.8% among patients referred for echocardiographic assessment. These patients are younger and show a higher frequency of previous myocardial infarction than those with severe AS randomized to TAVR in recent trials. In two retrospective studies including patients with moderate AS and reduced LVEF, a one-year mortality rate of 9 and 32% was reported, the latter in patients treated with medical therapy only during follow-up. Echocardiographic diagnosis of moderate AS poses challenges as current guidelines are directed to determine severe AS, and different presentations of moderate and mild AS have been generally neglected. Thus, the nomenclature would need to be revised and a description of possible scenarios is provided in this review. Dobutamine stress echocardiography and computed tomography are promising complementary tools. Likewise, a standardized clinical pathway is needed, in which a high level of suspicion and a low threshold for referral to a heart valve center is warranted. The Transcatheter Aortic Valve Replacement to UNload the Left ventricle in patients with Advanced heart failure (TAVR UNLOAD) trial (NCT02661451) is exploring whether TAVR would improve outcomes in patients receiving optimal heart failure therapy.
Keywords: TAVR UNLOAD trial; left ventricular ejection fraction; moderate aortic stenosis; structural heart disease; surgical aortic valve replacement; transcatheter aortic valve replacement.
Figures
Similar articles
-
Rationale and design of the Transcatheter Aortic Valve Replacement to UNload the Left ventricle in patients with ADvanced heart failure (TAVR UNLOAD) trial.Am Heart J. 2016 Dec;182:80-88. doi: 10.1016/j.ahj.2016.08.009. Epub 2016 Aug 26. Am Heart J. 2016. PMID: 27914503 Clinical Trial.
-
Outcomes From Transcatheter Aortic Valve Replacement in Patients With Low-Flow, Low-Gradient Aortic Stenosis and Left Ventricular Ejection Fraction Less Than 30%: A Substudy From the TOPAS-TAVI Registry.JAMA Cardiol. 2019 Jan 1;4(1):64-70. doi: 10.1001/jamacardio.2018.4320. JAMA Cardiol. 2019. PMID: 30566185 Free PMC article. Clinical Trial.
-
Moderate Aortic Stenosis and Heart Failure With Reduced Ejection Fraction: Can Imaging Guide Us to Therapy?JACC Cardiovasc Imaging. 2019 Jan;12(1):172-184. doi: 10.1016/j.jcmg.2018.10.021. JACC Cardiovasc Imaging. 2019. PMID: 30621989 Review.
-
Outcomes of transcatheter and surgical aortic valve replacement in high-risk patients with aortic stenosis and left ventricular dysfunction: results from the Placement of Aortic Transcatheter Valves (PARTNER) trial (cohort A).Circ Cardiovasc Interv. 2013 Dec;6(6):604-14. doi: 10.1161/CIRCINTERVENTIONS.113.000650. Epub 2013 Nov 12. Circ Cardiovasc Interv. 2013. PMID: 24221391 Clinical Trial.
-
Valvular performance and aortic regurgitation following transcatheter aortic valve replacement using Edwards valve versus CoreValve for severe aortic stenosis: A Meta-analysis.Cardiovasc Revasc Med. 2016 Jun;17(4):248-55. doi: 10.1016/j.carrev.2016.02.007. Epub 2016 Feb 19. Cardiovasc Revasc Med. 2016. PMID: 26948087 Review.
Cited by
-
Calculation of Aortic VAlve and LVOT Areas by a Modified Continuity Equation Using Different Echocardiography Methods: The CAVALIER Study.Diagnostics (Basel). 2022 Jul 7;12(7):1656. doi: 10.3390/diagnostics12071656. Diagnostics (Basel). 2022. PMID: 35885559 Free PMC article.
-
Unraveling the Enigma of Moderate Aortic Stenosis: Challenges and Future Prospects.J Clin Med. 2024 Jun 14;13(12):3478. doi: 10.3390/jcm13123478. J Clin Med. 2024. PMID: 38930005 Free PMC article. Review.
-
Impact of chronic kidney disease on long-term outcome of patients with valvular heart defects.Int Urol Nephrol. 2020 Nov;52(11):2161-2170. doi: 10.1007/s11255-020-02561-4. Epub 2020 Jul 14. Int Urol Nephrol. 2020. PMID: 32661631 Free PMC article.
-
Transcatheter and surgical aortic valve replacement in patients with left ventricular dysfunction.J Cardiothorac Surg. 2022 Dec 18;17(1):322. doi: 10.1186/s13019-022-02061-9. J Cardiothorac Surg. 2022. PMID: 36529781 Free PMC article. Clinical Trial.
References
-
- Osnabrugge RL, Mylotte D, Head SJ, Van Mieghem NM, Nkomo VT, Lereun CM, et al. . Aortic stenosis in the elderly: disease prevalence and number of candidates for transcatheter aortic valve replacement: a meta-analysis and modeling study. J Am Coll Cardiol. (2013) 62:1002–12. 10.1016/j.jacc.2013.05.015 - DOI - PubMed
-
- Smith WT, Ferguson TB Jr, Ryan T, Landolfo CK, Peterson ED. Should coronary artery bypass graft surgery patients with mild or moderate aortic stenosis undergo concomitant aortic valve replacement? A decision analysis approach to the surgical dilemma. J Am Coll Cardiol. (2004) 44:1241–7. 10.1016/j.jacc.2004.06.031 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials