

Meniscal Root Tears: Current Concepts Review
- PMID: 30175171
- PMCID: PMC6110430
Meniscal Root Tears: Current Concepts Review
Abstract
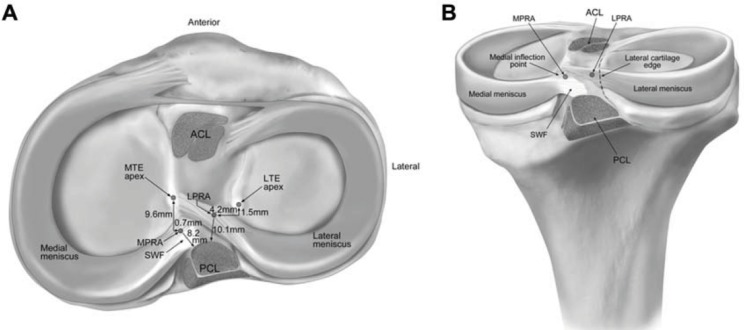
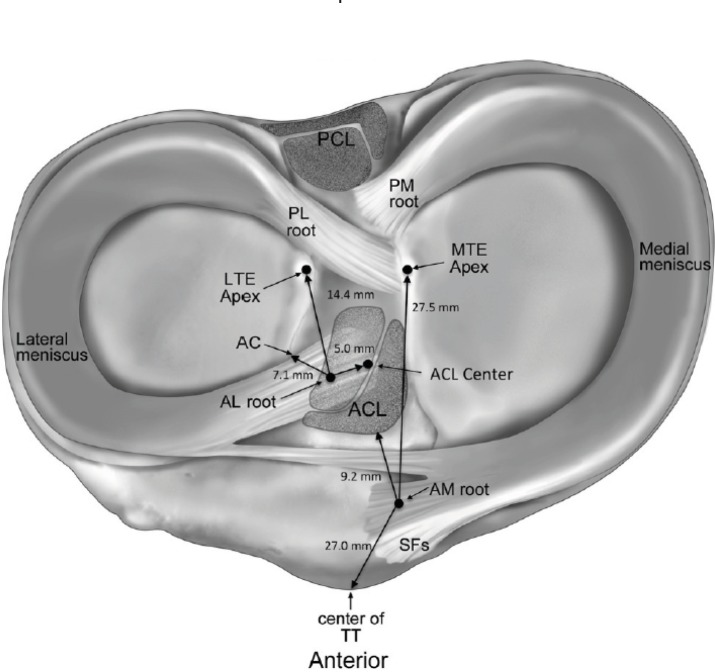
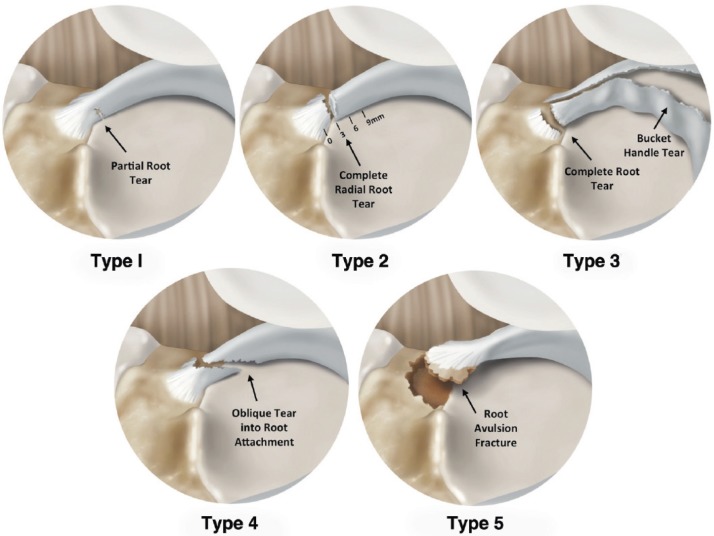
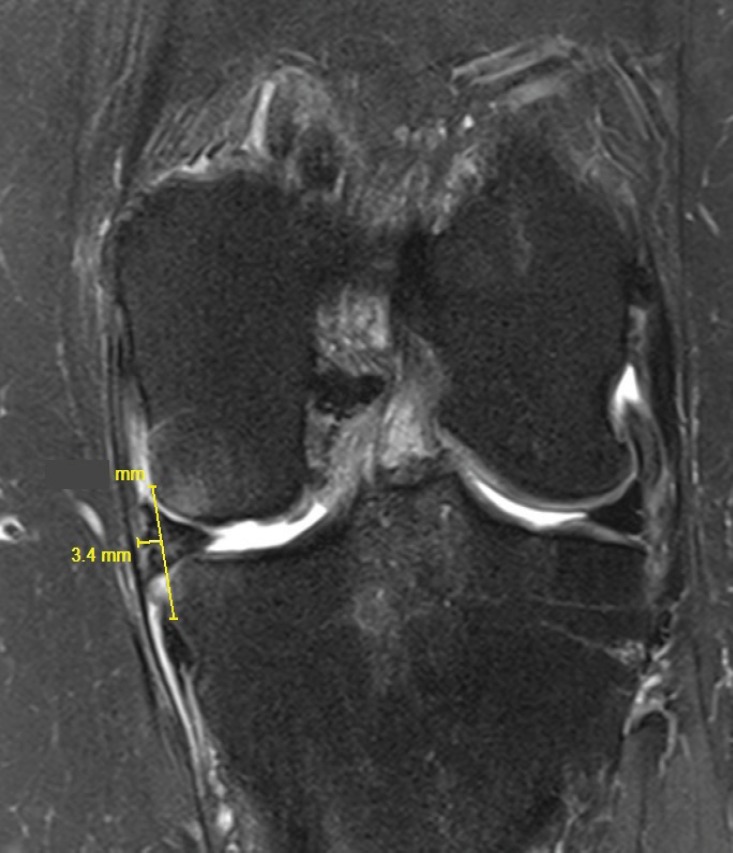
Meniscal root tears are defined as radial tears located within 1 cm from the meniscal attachment or a bony root avulsion. This injury is biomechanically comparable to a total meniscectomy, leading to compromised hoop stresses resulting in decreased tibiofemoral contact area and increased contact pressures in the involved compartment. These changes are detrimental to the articular cartilage and ultimately lead to the development of early osteoarthritis. Surgical repair is the treatment of choice in patients without significant osteoarthritis (Outerbridge grades 3 or 4). Root repairs have been reported to improve clinical outcomes, decrease meniscal extrusion and slow the onset of degenerative changes. Here we describe the anatomy, biomechanics, clinical evaluation, treatment methods, outcomes, and post-operative rehabilitation for posterior meniscal root tears.
Keywords: Lateral meniscus; Medial meniscus; Meniscus root tear; Outcomes; Root repair.
Figures

References
-
- Choi CJ, Choi YJ, Lee JJ, Choi CH. Magnetic resonance imaging evidence of meniscal extrusion in medial meniscus posterior root tear. Arthroscopy. 2010;26(12):1602–6. - PubMed
-
- Laprade CM, Jansson KS, Dornan G, Smith SD, Wijdicks CA, Laprade RF. Altered tibiofemoral contact mechanics due to lateral meniscus posterior horn root avulsions and radial tears can be restored with in situ pull-out suture repairs. J Bone Joint Surg Am. 2014;96(6):471–9. - PubMed
-
- Padalecki JR, Jansson KS, Smith SD, Dornan GJ, Pierce CM, Wijdicks CA, et al. Biomechanical consequences of a complete radial tear adjacent to the medial meniscus posterior root attachment site: in situ pull-out repair restores derangement of joint mechanics. Am J Sports Med. 2014;42(3):699–707. - PubMed
-
- Marzo JM, Gurske-DePerio J. Effects of medial meniscus posterior horn avulsion and repair on tibiofemoral contact area and peak contact pressure with clinical implications. Am J Sports Med. 2009;37(1):124–9. - PubMed
-
- Koenig JH, Ranawat AS, Umans HR, Difelice GS. Meniscal root tears: diagnosis and treatment. Arthroscopy. 2009;25(9):1025–32. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources