

Early Results of Oxford Mobile Bearing Medial Unicompartmental Knee Replacement (UKR) with the Microplasty Instrumentation: An Indian Experience
- PMID: 30175178
- PMCID: PMC6110431
Early Results of Oxford Mobile Bearing Medial Unicompartmental Knee Replacement (UKR) with the Microplasty Instrumentation: An Indian Experience
Abstract
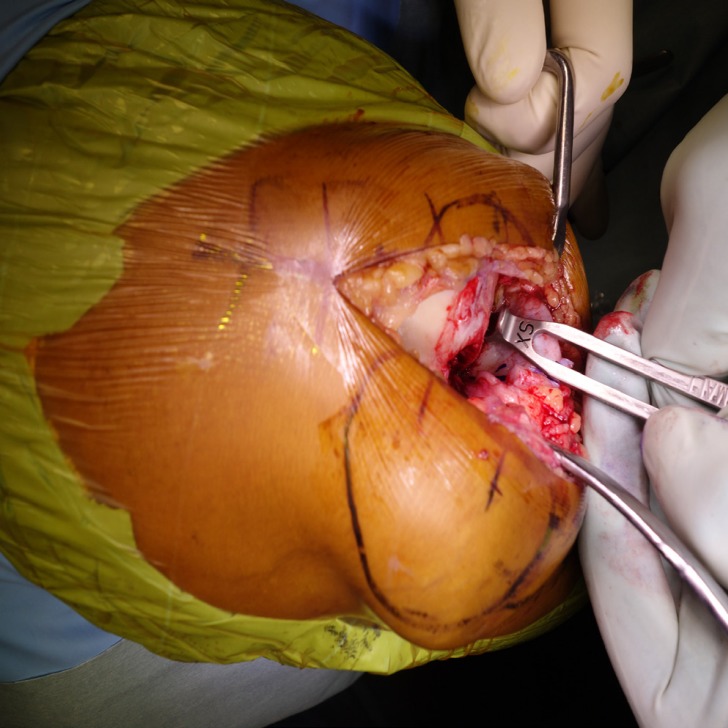
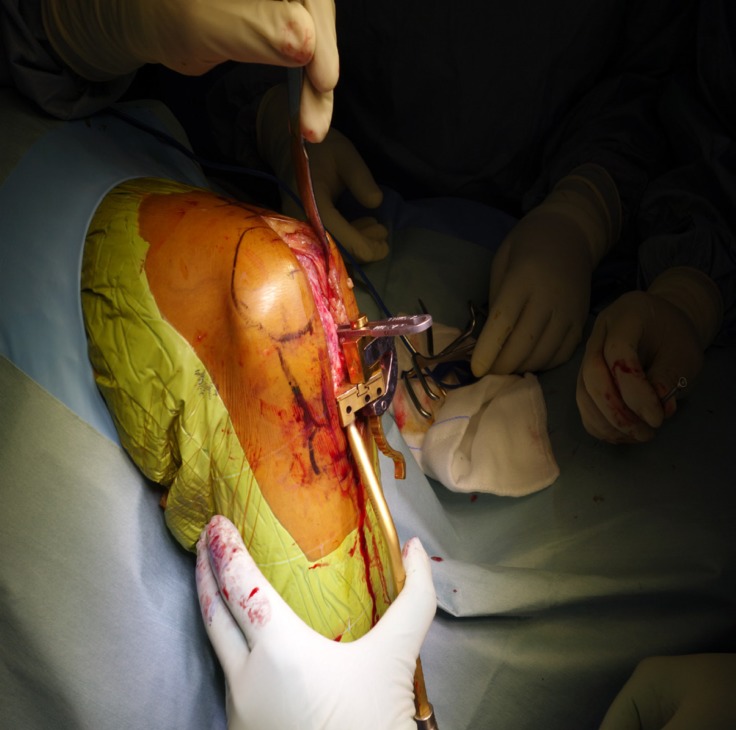
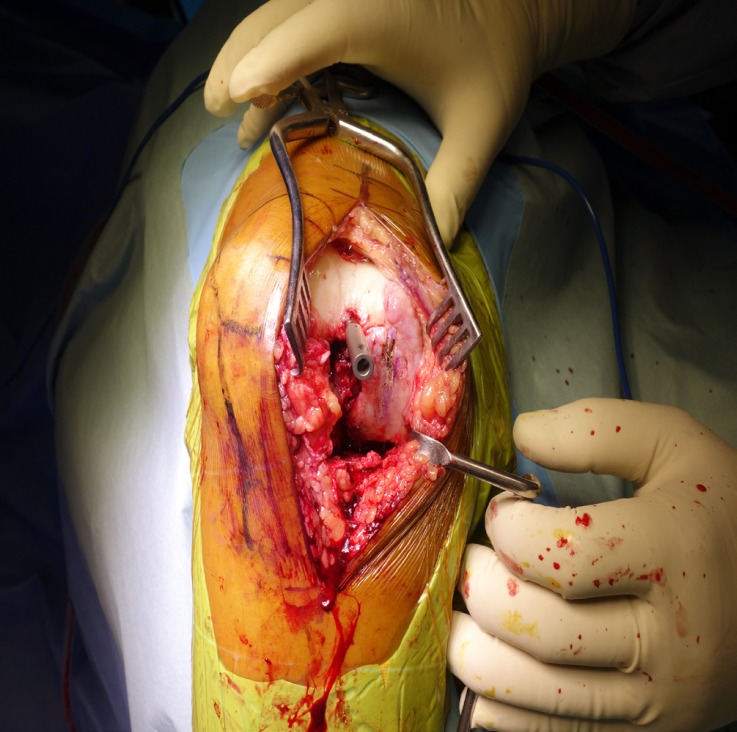
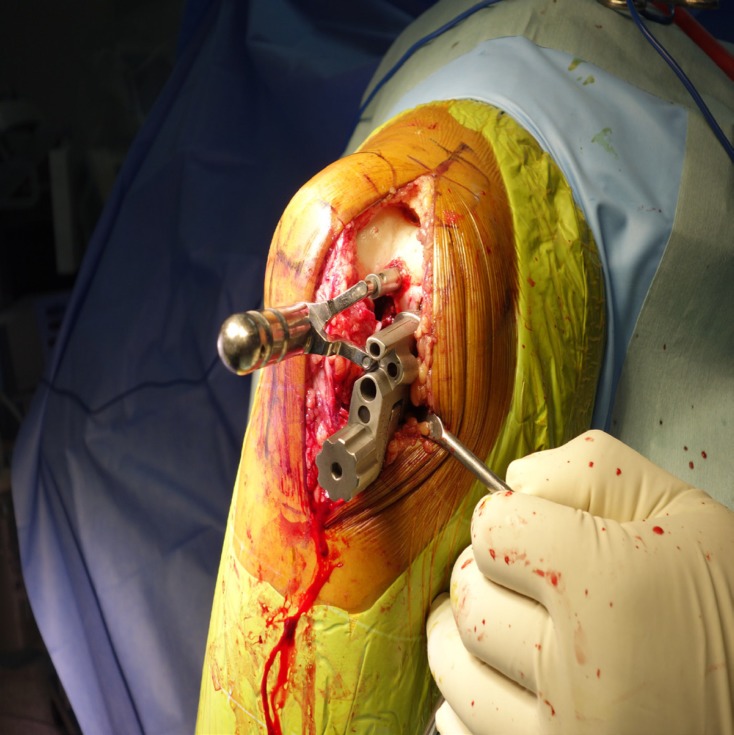
Background: Oxford medial unicompartmental knee replacement (UKR) is indicated in patients with anteromedial osteoarthritis (AMOA) of the knee. Microplasty (MP) instrumentation was introduced in 2012 as an improvement over phase 3 instrumentation. Advantages of this instrumentation include conservative tibial cut, decreased tibial re-cut rate and improved component alignment. We report the results of UKR with the new instrumentation in a consecutive series with a minimum follow-up of 2 years.
Methods: A prospective study of 115 cemented medial Oxford UKRs implanted in 89 patients was done. Post-operative alignment of the tibial and femoral components was analysed. Patient reported outcome measures were recorded using Oxford Knee Score (OKS) and the American Knee Society Score (KSS). Tegner Activity Scale (TAS) was used to record the activity level.
Results: 115 consecutive medial Oxford UKRs were studied. All patients were followed up annually in this prospective ethically approved study. The mean follow-up was 36 months and the minimum follow-up was 25 months. No patient died and none were lost to follow-up. At the final follow-up, the average OKS of the cohort was 39.5 (SD: 5.7). 91.2 % of the patients had good or excellent OKS with only 3.5 % reporting poor OKS. The overall limb alignment was 4.80 varus (0 - 140 varus). Tibia was recut in 5.2 % of cases. Median bearing size was 3 (range: 3 to 6). There was one case of bearing dislocation and one case of aseptic tibial loosening.
Conclusion: This is the first study to report results of MP instrumentation at a minimum follow-up of 2 years. Our study indicates that the new instrumentation results in reliable and accurate implantation of femoral and tibial components in majority of the cases, with a decrease in number of alignment outliers, and also a reduced rate of bearing dislocation.
Keywords: Anteromedial osteoarthritis (AMOA); Microplasty instrumentation; Mobile bearing; Unicompartmental knee replacement (UKR).
Figures


Similar articles
-
Does new instrument for Oxford unicompartmental knee arthroplasty improve short-term clinical outcome and component alignment? A meta-analysis.J Orthop Surg Res. 2020 Sep 7;15(1):386. doi: 10.1186/s13018-020-01926-w. J Orthop Surg Res. 2020. PMID: 32894147 Free PMC article. Review.
-
[Accuracy of Alignment of Femoral and Tibial Component of the Oxford Medial Unicompartmental Knee Arthroplasty Using Zimmer Microplasty® Instrumentation].Acta Chir Orthop Traumatol Cech. 2021;88(4):291-301. Acta Chir Orthop Traumatol Cech. 2021. PMID: 34534059 Czech.
-
Fixed lateral unicompartmental knee replacement is a reliable treatment for lateral compartment osteoarthritis after mobile-bearing medial unicompartmental replacement.Knee Surg Sports Traumatol Arthrosc. 2023 Dec;31(12):5407-5412. doi: 10.1007/s00167-023-07573-y. Epub 2023 Sep 28. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 37768357 Free PMC article.
-
Can accuracy of component alignment be improved with Oxford UKA Microplasty® instrumentation?J Orthop Surg Res. 2020 Aug 26;15(1):354. doi: 10.1186/s13018-020-01868-3. J Orthop Surg Res. 2020. PMID: 32843044 Free PMC article.
-
Accuracy and early outcomes in medial unicompartmental knee arthroplasty performed using patient specific instrumentation.Knee. 2014;21 Suppl 1:S33-6. doi: 10.1016/S0968-0160(14)50007-5. Knee. 2014. PMID: 25382366 Review.
Cited by
-
The association between surgeon grade and radiographic implant alignment following oxford unicompartmental knee replacement.Arch Orthop Trauma Surg. 2025 Jul 3;145(1):362. doi: 10.1007/s00402-025-05973-y. Arch Orthop Trauma Surg. 2025. PMID: 40608142 Free PMC article.
-
Does new instrument for Oxford unicompartmental knee arthroplasty improve short-term clinical outcome and component alignment? A meta-analysis.J Orthop Surg Res. 2020 Sep 7;15(1):386. doi: 10.1186/s13018-020-01926-w. J Orthop Surg Res. 2020. PMID: 32894147 Free PMC article. Review.
-
No difference in the use of revision components and rerevision rate in conversion to total knee replacement following Oxford Partial Knee Microplasty Instrumentation: a registry study of 529 conversions.Acta Orthop. 2023 Jul 31;94:387-392. doi: 10.2340/17453674.2023.15310. Acta Orthop. 2023. PMID: 37519250 Free PMC article.
References
-
- White SH, Ludkowski PF, Goodfellow JW. Anteromedial osteoarthritis of the knee. J Bone Joint Surg Br. 1991;73(4):582–6. - PubMed
-
- Goodfellow JW, O’Connor J. Clinical results of the Oxford knee Surface arthroplasty of the tibiofemoral joint with a meniscal bearing prosthesis. Clin Orthop Relat Res. 1986;205(1):21–42. - PubMed
-
- Price AJ, O’Connor JJ, Murray DW, Dodd CA, Goodfellow JW. A history of Oxford unicompartmental knee arthroplasty. Orthopedics. 2007;30(5 Suppl):7–10. - PubMed
-
- Hurst JM, Berend KR. Mobile-bearing unicondylar knee arthroplasty: the Oxford experience. Orthop Clin North Am. 2015;46(1):113–24. - PubMed
LinkOut - more resources
Full Text Sources