

Burden of dengue among febrile patients at the time of chikungunya introduction in Piedecuesta, Colombia
- PMID: 30176107
- PMCID: PMC6334506
- DOI: 10.1111/tmi.13147
Burden of dengue among febrile patients at the time of chikungunya introduction in Piedecuesta, Colombia
Abstract
Objective: To estimate the age-specific incidence of symptomatic dengue and chikungunya in Colombia.
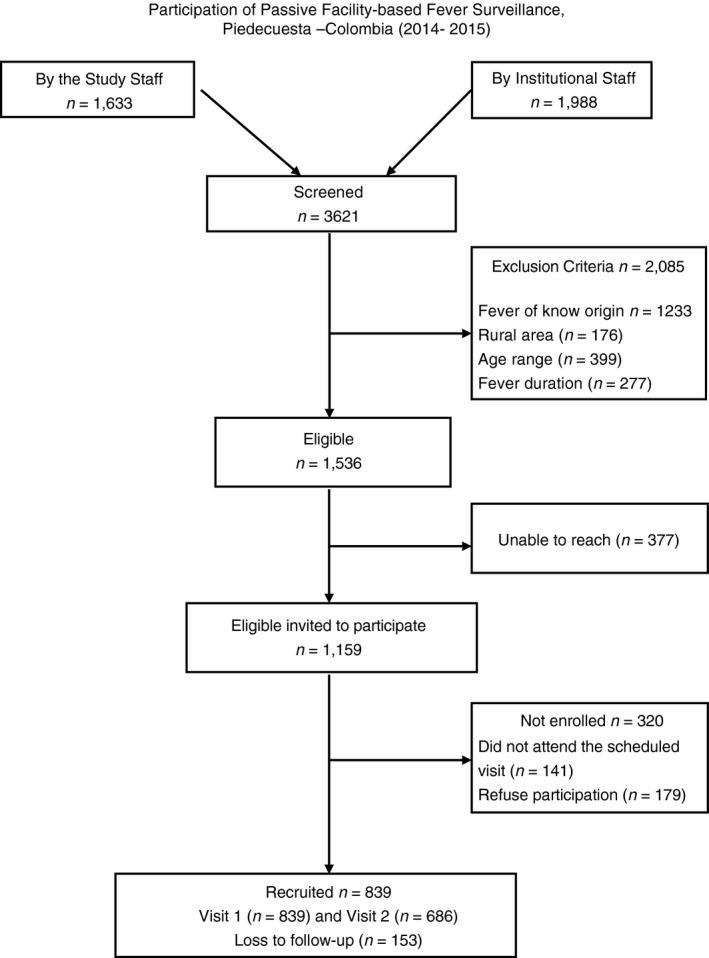
Method: A passive facility-based fever surveillance study was conducted among individuals with undifferentiated fever. Confirmatory diagnostics included serological and molecular tests in paired samples, and surveillance's underreporting was assessed using capture-recapture methods.
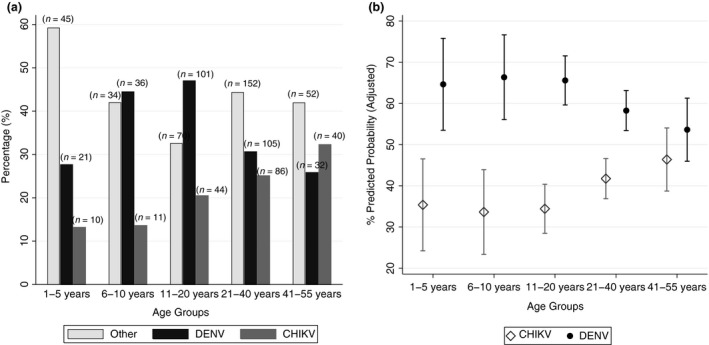
Results: Of 839 febrile participants 686 completed the study. There were 33.2% (295/839) dengue infections (51% primary infections), and 35.9% (191/532) of negative dengue cases there were chikungunya cases. On average, dengue cases were younger (median = 18 years) than chikungunya cases (median = 25 years). Thrombocytopaenia and abdominal pain were the main dengue predictors, while presence of rash was the main predictor for chikungunya diagnosis. Underreporting of dengue was 31%; the estimated expansion factors indicate an underreporting rate of dengue cases of threefold for all cases and of almost sixfold for inpatients.
Conclusions: These findings highlight the ongoing coexistence of both arboviruses, a distinct clinical profile of each condition in the study area that could be used by clinicians to generate a differential diagnosis, and the presence of underreporting, mostly among hospitalised cases.
Objectif: Estimer l'incidence selon l’âge de la dengue et du chikungunya symptomatiques en Colombie.
Méthode: Une étude de surveillance passive de la fièvre dans les établissements a été menée auprès d'individus présentant une fièvre indifférenciée. Les diagnostics de confirmation comprenaient des tests sérologiques et moléculaires sur des échantillons appariés et la sous‐déclaration dans la surveillance a été évaluée à l'aide de méthodes de capture‐recapture.
Résultats: Sur 839 participants fébriles, 686 ont terminé l’étude. Il y avait 33,2% (295/839) d'infections à la dengue (51% d'infections primaires) et 35,9% (191/532) des cas négatifs pour la dengue étaient des cas de chikungunya. En moyenne, les cas de dengue étaient plus jeunes (médiane = 18 ans) que les cas de chikungunya (médiane = 25 ans). La thrombocytopénie et les douleurs abdominales étaient les principaux facteurs prédictifs de la dengue, tandis que la présence d’éruptions cutanées était le principal facteur prédictif du diagnostic du chikungunya. La sous‐déclaration de la dengue était de 31%; les facteurs d'expansion estimés indiquent un taux de sous‐déclaration des cas de dengue de 3 fois pour tous les cas et de presque 6 fois pour les patients hospitalisés.
Conclusions: Ces résultats mettent en évidence la coexistence continue des deux arbovirus, un profil clinique distinct de chaque condition dans la zone d’étude qui pourrait être utilisé par les cliniciens pour générer un diagnostic différentiel et la présence de sous‐déclaration, principalement parmi les cas hospitalisés.
Keywords: Colombia; Colombie; caractérisation clinique; chikungunya; clinical characterisation; dengue; disease incidence; fever surveillance; incidence de la maladie; sous-déclaration; surveillance de la fièvre; underreporting.
© 2018 The Authors. Tropical Medicine & International Health Published by John Wiley & Sons Ltd.
Figures
References
-
- World Health Organization (WHO) . Dengue: prevention and control. In: Sixty‐eight World Health Assembly. Geneva, Switzerland: World Health Organization; 2015.
-
- Rodriguez‐Morales AJ, Villamil‐Gómez WE, Franco‐Paredes C. The arboviral burden of disease caused by co‐circulation and co‐infection of dengue, chikungunya and Zika in the Americas. Travel Med Infect Dis 2016: 14: 177–179. - PubMed
-
- World Health Organization (WHO) . Dengue vaccine: WHO position paper – July 2016 In: Weekly Epidemiological Record, Vol. 91, WHO edn World Health Organization: Geneva, 2016; 349–364. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
