

Treatment of mycophenolate-resistant immune-related organizing pneumonia with infliximab
- PMID: 30176946
- PMCID: PMC6122461
- DOI: 10.1186/s40425-018-0400-4
Treatment of mycophenolate-resistant immune-related organizing pneumonia with infliximab
Abstract
Background: The development of pulmonary immune-related adverse events (irAEs) in patients undergoing PD-(L)1 targeted checkpoint inhibitors are rare, but may be life-threatening. While many published articles and guidelines are focusing on the presentation and upfront treatment of pulmonary irAEs, the strategy in patients with late-onset pneumonia that are resistant to commonly used immunosuppressive drugs remains unclear.
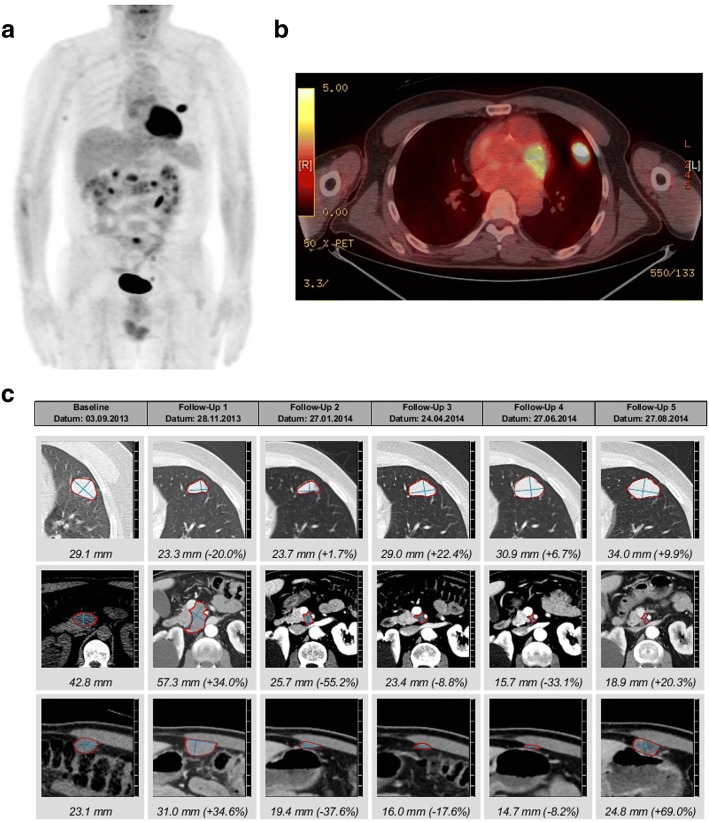
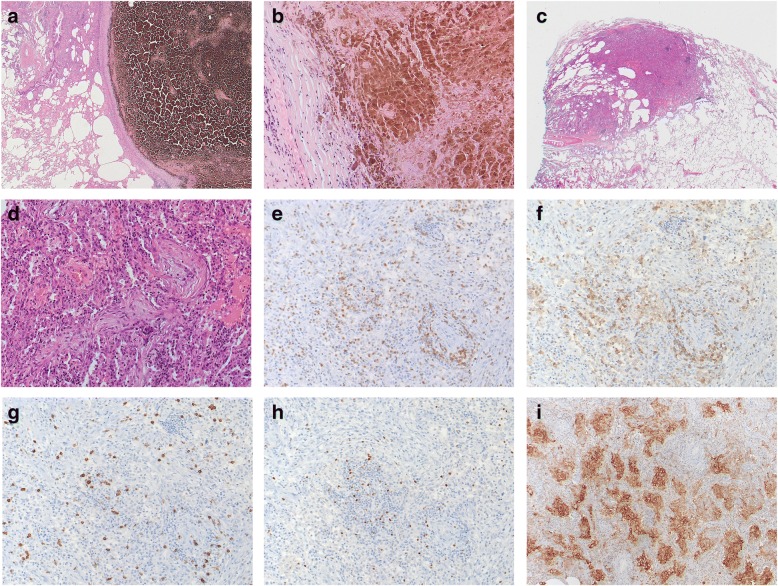
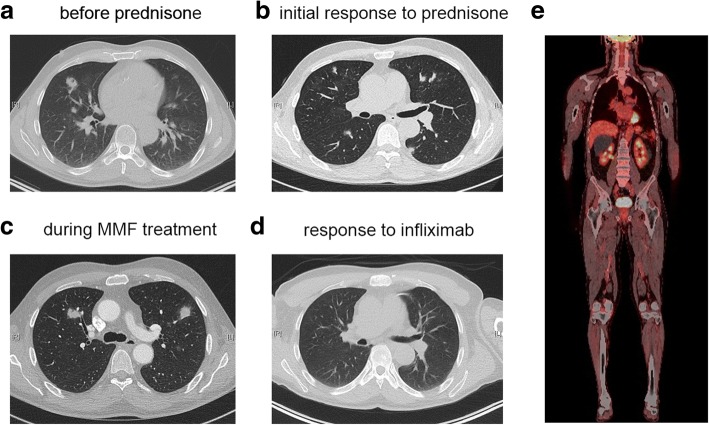
Case presentation: Here, we report the successful treatment of a mycophenolate-resistant organizing pneumonia (OP) with infliximab in a patient with metastatic melanoma after PD-1 blockade. The patient received two years of PD-1 targeted immunotherapy when he developed multiple nodular lung lesions mimicking a metastatic progression. However, wedge resection of these lesions showed defined areas of OP, which responded well to corticosteroids. Upon tapering, new foci of OP developed which were resistant to high-dose steroids and mycophenolate treatment. The TNFα antagonist infliximab led to a rapid and durable regression of the inflammatory lesions.
Conclusion: This case describes a not well-studied situation, in which a mycophenolate-resistant PD-1 blocker-associated pneumonitis was successfully treated with a TNFα neutralizing antibody. The outcome of this case suggests that infliximab might be the preferable option compared to classical immunosuppressants in the case of steroid-resistant/-dependent late onset pulmonary irAEs.
Keywords: Cancer immunotherapy; Immune checkpoint inhibitor; Immune-related adverse event; Lung; Pneumonitis.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was obtained from the local ethical committee to analyze the tissue and blood samples. Written informed consent was obtained from the patient for the analysis of the samples and the tissue.
Consent for publication
A consent for publication was obtained from the patient. A copy of the written consent is available for review.
Competing interests
H.L., and A.Z. received travel grants and consultant fees from Bristol-Myers Squibb (BMS) and Merck, Sharp and Dohme (MSD).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Heinzerling L, Goldinger SM. A review of serious adverse effects under treatment with checkpoint inhibitors. Curr Opin Oncol. 2017;29(2):136–144. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous