

Gastrointestinal Symptoms and Oral Antibiotic Use in Children with Autism Spectrum Disorder: Retrospective Analysis of a Privately Insured U.S. Population
- PMID: 30178105
- PMCID: PMC6365214
- DOI: 10.1007/s10803-018-3743-2
Gastrointestinal Symptoms and Oral Antibiotic Use in Children with Autism Spectrum Disorder: Retrospective Analysis of a Privately Insured U.S. Population
Abstract
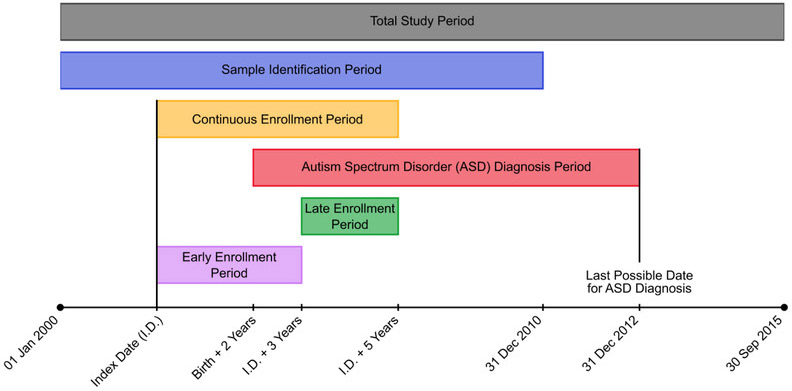
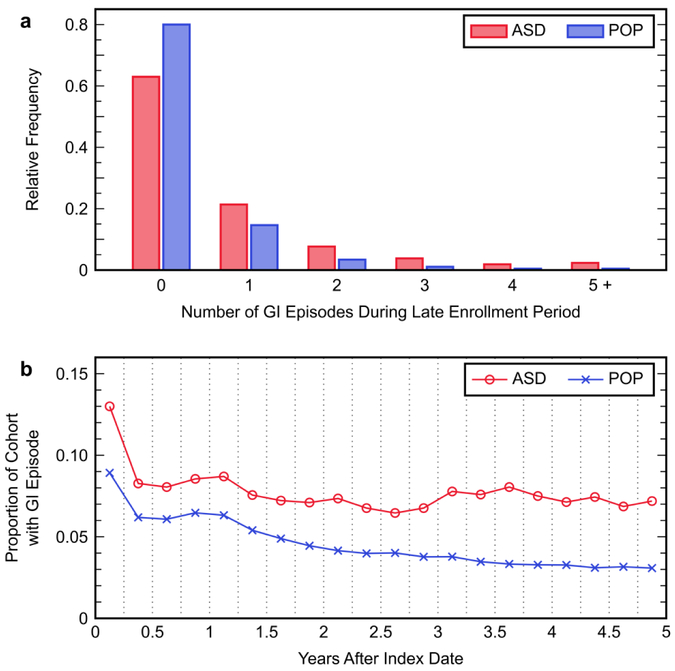
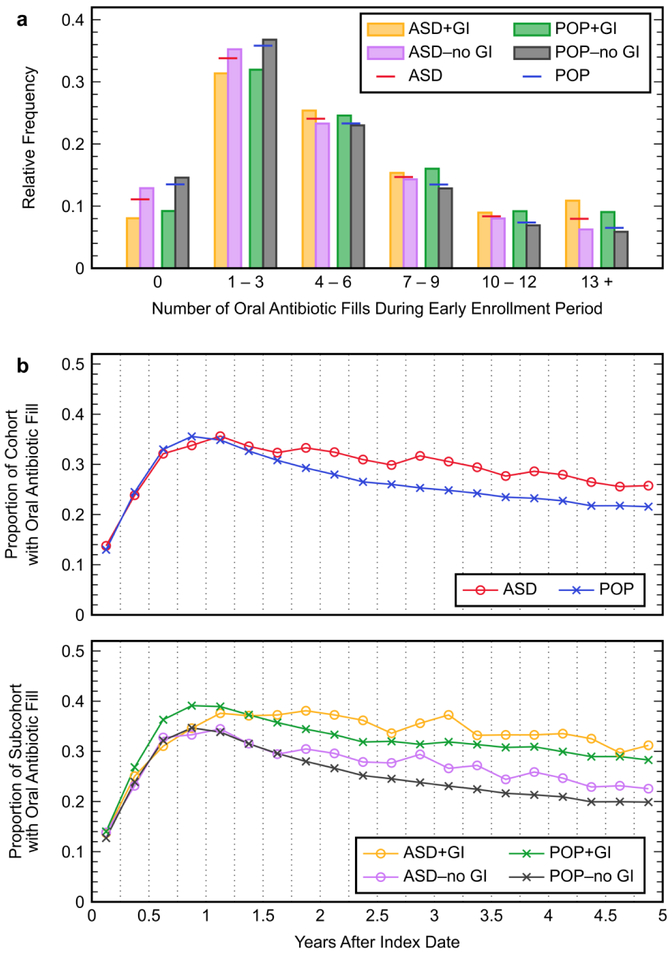
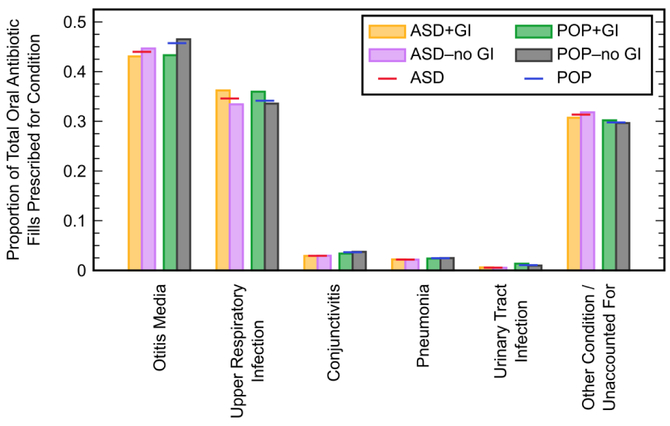
A retrospective analysis of administrative claims data from a large U.S. health insurer was performed to study a potential association between oral antibiotic use during early childhood and occurrence of later gastrointestinal (GI) symptoms in children with autism spectrum disorder (ASD). Among 3253 children with ASD, 37.0% had a GI-related diagnosis during the last 2 years of their 5-year health coverage enrollment period, compared to 20.0% of 278,370 children from the general population without an ASD diagnosis. Greater numbers of oral antibiotic fills during the first 3 years of enrollment were found to significantly increase the hazard rate of having a later GI-related diagnosis (adjusted hazard ratio 1.48; 95% confidence interval 1.34, 1.63) in children both with and without ASD.
Keywords: Administrative claims; Autism spectrum disorder; Gastrointestinal symptoms; Gut microbiome; Oral antibiotics; Retrospective analysis.
Conflict of interest statement
Conflict of Interest: The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Effects of gut microbial-based treatments on gut microbiota, behavioral symptoms, and gastrointestinal symptoms in children with autism spectrum disorder: A systematic review.Psychiatry Res. 2020 Nov;293:113471. doi: 10.1016/j.psychres.2020.113471. Epub 2020 Sep 26. Psychiatry Res. 2020. PMID: 33198044
-
Early childhood antibiotics use and autism spectrum disorders: a population-based cohort study.Int J Epidemiol. 2018 Oct 1;47(5):1497-1506. doi: 10.1093/ije/dyy162. Int J Epidemiol. 2018. PMID: 30101312
-
Gut to brain interaction in Autism Spectrum Disorders: a randomized controlled trial on the role of probiotics on clinical, biochemical and neurophysiological parameters.BMC Psychiatry. 2016 Jun 4;16:183. doi: 10.1186/s12888-016-0887-5. BMC Psychiatry. 2016. PMID: 27260271 Free PMC article. Clinical Trial.
-
Brief Report: Association Between Autism Spectrum Disorder, Gastrointestinal Problems and Perinatal Risk Factors Within Sibling Pairs.J Autism Dev Disord. 2017 Aug;47(8):2621-2627. doi: 10.1007/s10803-017-3169-2. J Autism Dev Disord. 2017. PMID: 28536957
-
Microbiota and gut-brain axis dysfunction in autism spectrum disorder: Evidence for functional gastrointestinal disorders.Asian J Psychiatr. 2020 Jan;47:101874. doi: 10.1016/j.ajp.2019.101874. Epub 2019 Nov 12. Asian J Psychiatr. 2020. PMID: 31785441 Review.
Cited by
-
Autism spectrum disorders and the gastrointestinal tract: insights into mechanisms and clinical relevance.Nat Rev Gastroenterol Hepatol. 2024 Mar;21(3):142-163. doi: 10.1038/s41575-023-00857-1. Epub 2023 Dec 19. Nat Rev Gastroenterol Hepatol. 2024. PMID: 38114585 Review.
-
The Difference of Gut Microbiota and Their Correlations With Urinary Organic Acids Between Autistic Children With and Without Atopic Dermatitis.Front Cell Infect Microbiol. 2022 Jun 21;12:886196. doi: 10.3389/fcimb.2022.886196. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 35800387 Free PMC article.
-
Predicting Problematic Behavior in Autism Spectrum Disorder Using Medical History and Environmental Data.J Pers Med. 2023 Oct 21;13(10):1513. doi: 10.3390/jpm13101513. J Pers Med. 2023. PMID: 37888124 Free PMC article.
-
Pregnant Mothers' Medical Claims and Associated Risk of Their Children being Diagnosed with Autism Spectrum Disorder.J Pers Med. 2021 Sep 24;11(10):950. doi: 10.3390/jpm11100950. J Pers Med. 2021. PMID: 34683092 Free PMC article.
-
Overall Rebalancing of Gut Microbiota Is Key to Autism Intervention.Front Psychol. 2022 May 26;13:862719. doi: 10.3389/fpsyg.2022.862719. eCollection 2022. Front Psychol. 2022. PMID: 35712154 Free PMC article. Review.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
