

Do patient-specific instruments (PSI) for UKA allow non-expert surgeons to achieve the same saw cut accuracy as expert surgeons?
- PMID: 30178169
- PMCID: PMC6182679
- DOI: 10.1007/s00402-018-3031-9
Do patient-specific instruments (PSI) for UKA allow non-expert surgeons to achieve the same saw cut accuracy as expert surgeons?
Abstract
Introduction: High-volume unicompartmental knee arthroplasty (UKA) surgeons have lower revision rates, in part due to improved intra-operative component alignment. This study set out to determine whether PSI might allow non-expert surgeons to achieve the same level of accuracy as expert surgeons.
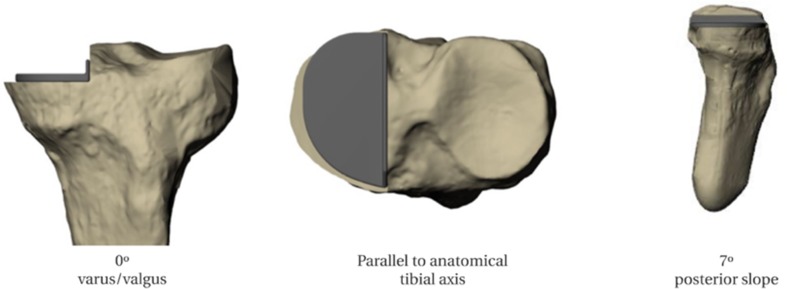
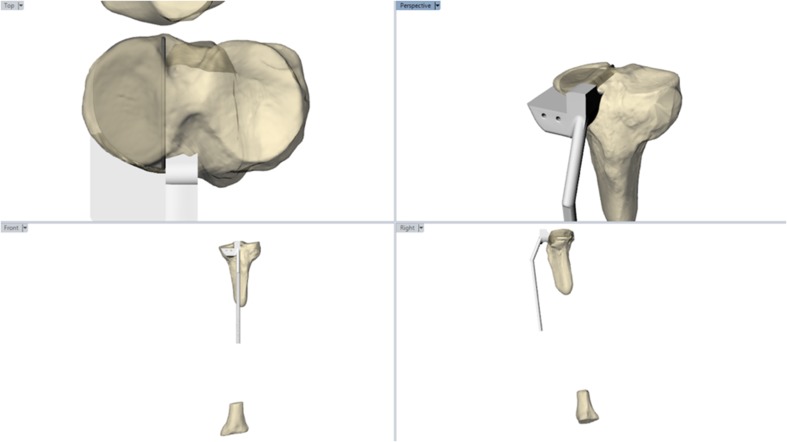
Materials and methods: Thirty-four surgical trainees with no prior experience of UKA, and four high-volume UKA surgeons were asked to perform the tibial saw cuts for a medial UKA in a sawbone model using both conventional and patient-specific instrumentation (PSI) with the aim of achieving a specified pre-operative plan. Half the participants in each group started with conventional instrumentation, and half with PSI. CT scans of the 76 cut sawbones were then segmented and reliably orientated in space, before saw cut position in the sagittal, coronal and axial planes was measured, and compared to the pre-operative plan.
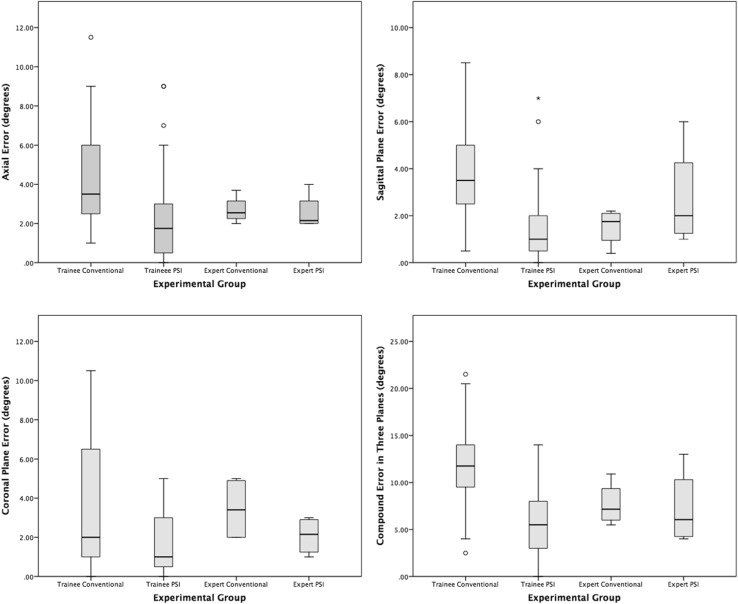
Results: The compound error (absolute error in the coronal, sagittal and axial planes combined) for experts using conventional instruments was significantly less than that of the trainees (11.6°±4.0° v 7.7° ±2.3º, p = 0.029). PSI improved trainee accuracy to the same level as experts using conventional instruments (compound error 5.5° ±3.4º v 7.7° ±2.3º, p = 0.396) and patient-specific instruments (compound error 5.5° ±3.4º v 7.3° ±4.1º, p = 0.3). PSI did not improve the accuracy of high-volume surgeons (p = 0.3).
Conclusions: In a sawbone model, PSI allowed inexperienced surgeons to achieve more accurate saw cuts, equivalent to expert surgeons, and thus has the potential to reduce revision rates. The next test will be to determine whether these results can be replicated in a clinical trial.
Keywords: 3D printing; PSI; Partial knee replacement; Patient-specific guides; Patient-specific instrumentation; Unicompartmental knee arthroplasty.
Conflict of interest statement
Conflict of interest
G. Jones declares grants from The Frances and Augustus Newman Foundation and from The Michael Uren Foundation, activity relating to the submitted work. S. Clarke declares provision of equipment from Embody Orthopaedic, activity relating to the submitted work; board membership, royalties and stocks/stock options from Embody Orthopaedic, activity outside the submitted work. M. Jaere declares consultancy for Embody Orthopaedic, activity outside the submitted work. S. Harris declares consultancy for Embody Orthopaedic, activity outside the submitted work. J. Cobb declares grant funding from the Michael Uren Foundation, activity relating to the submitted work; patents and stocks/stock options for Embody Orthopaedic, activity outside the submitted work.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures
References
-
- Green M, Wishart N, Young E, Mccormack V, Swanson M (2016) National Joint Registry for England, Wales, Northern Ireland and the Isle of Man 14th Annual Report 2017
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
