

A Survey of Expert Practice and Attitudes Regarding Advanced Imaging Modalities in Surveillance of Barrett's Esophagus
- PMID: 30178283
- PMCID: PMC6541486
- DOI: 10.1007/s10620-018-5257-3
A Survey of Expert Practice and Attitudes Regarding Advanced Imaging Modalities in Surveillance of Barrett's Esophagus
Abstract
Background: Published guidelines do not address what the minimum incremental diagnostic yield (IDY) for detection of dysplasia/cancer is required over the standard Seattle protocol for an advanced imaging modality (AIM) to be implemented in routine surveillance of Barrett's esophagus (BE) patients. We aimed to report expert practice patterns and attitudes, specifically addressing the minimum IDY in the use of AIMs in BE surveillance.
Methods: An international group of BE experts completed an anonymous electronic survey of domains relevant to surveillance practice patterns and use of AIMs. The evaluated AIMs were conventional chromoendoscopy (CC), virtual chromoendoscopy (VC), volumetric laser endomicroscopy (VLE), confocal laser endomicroscopy (CLE), and wide-area transepithelial sampling (WATS3D). Responses were recorded using five-point balanced Likert items and analyzed as continuous variables.
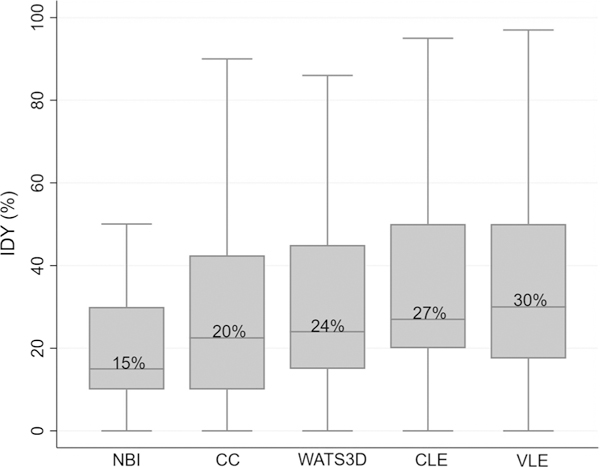
Results: The survey response rate was 84% (61/73)-41 US and 20 non-US. Experts were most comfortable with and routinely use VC and CC, and least comfortable with and rarely use VLE, CLE, and WATS3D. Experts rated data from randomized controlled trials (1.4 ± 0.9) and guidelines (2.6 ± 1.2) as the two most influential factors for implementing AIMs in clinical practice. The minimum IDY of AIMs over standard biopsies to be considered of clinical benefit was lowest for VC (15%, IQR 10-29%) and highest for VLE (30%, IQR 20-50%). Compared to US experts, non-US experts reported higher use of CC for BE surveillance (p < 0.001).
Conclusion: These results should inform benchmarks that need to be met for guidelines to recommend the routine use of AIMs in the surveillance of BE patients.
Keywords: Advanced imaging modalities; Barrett’s esophagus; Practice patterns; Surveillance.
Conflict of interest statement
Figures
References
-
- Pennathur A, Gibson MK, Jobe BA, et al. Oesophageal carcinoma. Lancet. 2013;381:400–412. - PubMed
-
- Cameron AJ, Carpenter HA. Barrett’s esophagus, high-grade dysplasia, and early adenocarcinoma: a pathological study. Am J Gastroenterol. 1997;92:586–591. - PubMed
-
- Fitzgerald RC, di Pietro M, Ragunath K, et al. British Society of Gastroenterology guidelines on the diagnosis and management of Barrett’s oesophagus. Gut. 2014;63:7–42. - PubMed
-
- Weusten B, Bisschops R, Coron E, et al. Endoscopic management of Barrett’s esophagus: European Society of Gastrointestinal Endoscopy (ESGE) position statement. Endoscopy. 2017;49:191–198. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
