

Data Rich, Information Poor: Can We Use Electronic Health Records to Create a Learning Healthcare System for Pharmaceuticals?
- PMID: 30178490
- PMCID: PMC6587701
- DOI: 10.1002/cpt.1226
Data Rich, Information Poor: Can We Use Electronic Health Records to Create a Learning Healthcare System for Pharmaceuticals?
Abstract
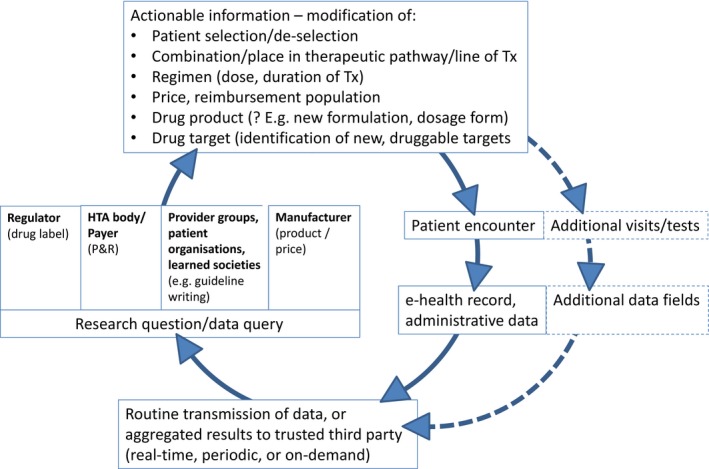
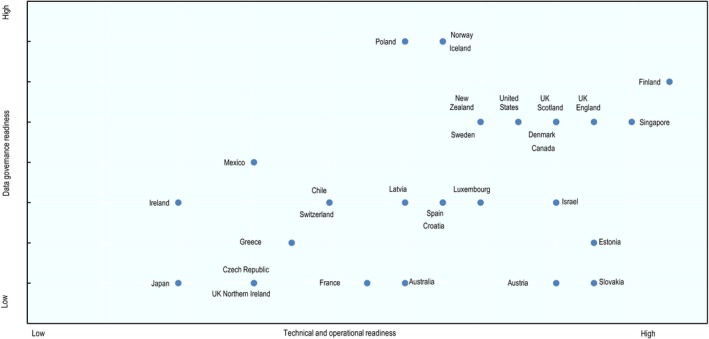
Judicious use of real-world data (RWD) is expected to make all steps in the development and use of pharmaceuticals more effective and efficient, including research and development, regulatory decision making, health technology assessment, pricing, and reimbursement decisions and treatment. A "learning healthcare system" based on electronic health records and other routinely collected data will be required to harness the full potential of RWD to complement evidence based on randomized controlled trials. We describe and illustrate with examples the growing demand for a learning healthcare system; we contrast the exigencies of an efficient pharmaceutical ecosystem in the future with current deficiencies highlighted in recently published Organisation for Economic Co-operation and Development (OECD) reports; and we reflect on the steps necessary to enable the transition from healthcare data to actionable information. A coordinated effort from all stakeholders and international cooperation will be required to increase the speed of implementation of the learning healthcare system, to everybody's benefit.
© 2018 The Authors Clinical Pharmacology & Therapeutics published by Wiley Periodicals, Inc. on behalf of American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
The authors declared no competing interests for this work.
Figures
References
-
- Oderkirk, J. Readiness of electronic health record systems to contribute to national health information and research. OECD Health Working Papers, No. 99 (OECD Publishing, Paris, 2017). < 10.1787/9e296bf3-en> - DOI
-
- OECD. Health Data Governance: Privacy, Monitoring and Research. OECD Publishing, Paris: (2015). < 10.1787/9789264244566-en>. - DOI
-
- IoM . The learning healthcare project website. <http://www.learninghealthcareproject.org/section/background/learning-hea...> (2015).
-
- ENCEPP Collaboration . European Network of Centres for Pharmacoepidemiology and Pharmacovigilance website. <http://www.encepp.eu/>.
-
- Sentinel initiative. <https://www.fda.gov/Safety/FDAsSentinelInitiative/ucm2007250.htm>
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
