

Association between carotid atheroma and cerebral cortex structure at age 73 years
- PMID: 30179274
- PMCID: PMC6328248
- DOI: 10.1002/ana.25324
Association between carotid atheroma and cerebral cortex structure at age 73 years
Abstract
Objective: To examine the relationship between carotid atherosclerosis and cerebral cortical thickness and investigate whether cortical thickness mediates the association between carotid atheroma and relative cognitive decline.
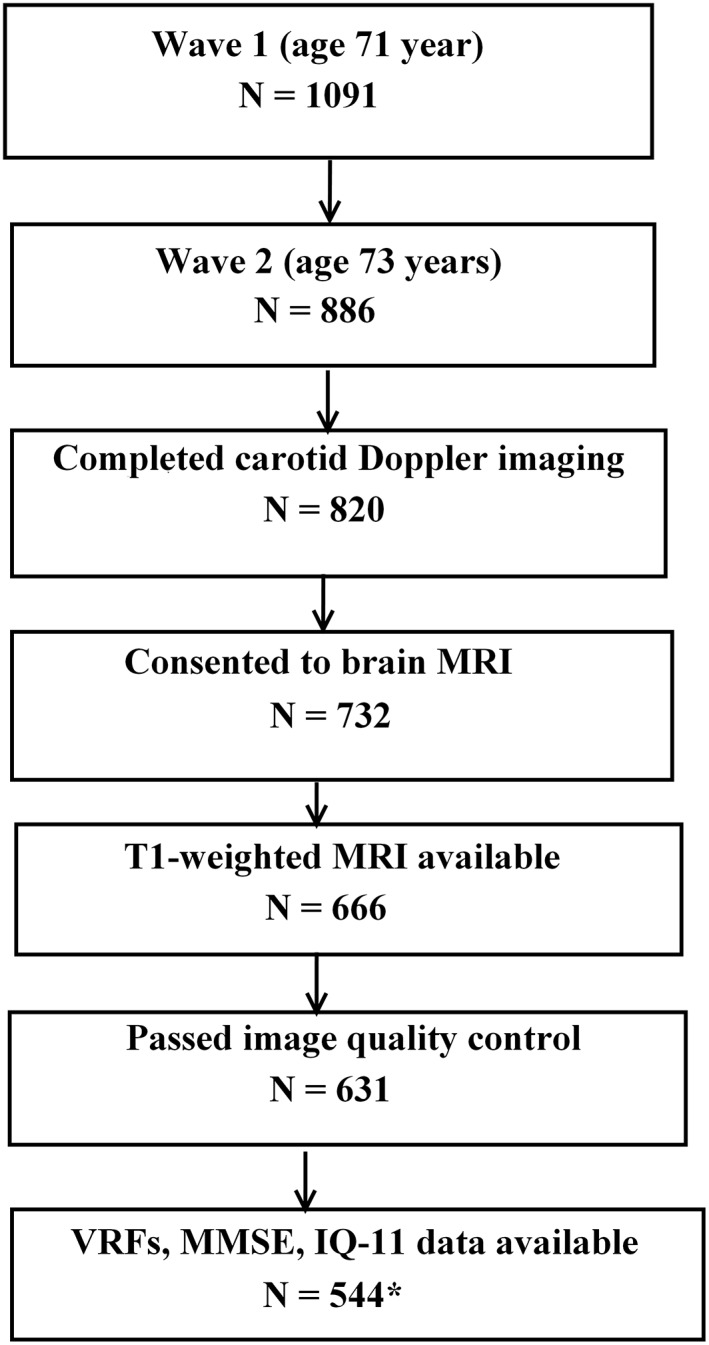
Methods: We assessed 554 community-dwelling subjects (male/female: 296/258) from the Lothian Birth Cohort 1936 who underwent brain magnetic resonance imaging and carotid Doppler ultrasound studies at age 73 years. The relationship between carotid atherosclerosis markers (internal carotid artery stenosis, intima-media thickness, velocity, pulsatility, and resistivity indexes) and vertex-wide cerebral cortical thickness was examined cross-sectionally, controlling for gender, extensive vascular risk factors (VRFs), and intelligence quotient at age 11 (IQ-11). We also determined the association between carotid stenosis and a composite measure of fluid intelligence at age 73 years. A mediation model was applied to examine whether cortical thickness mediated the relationship between carotid stenosis and cognitive function.
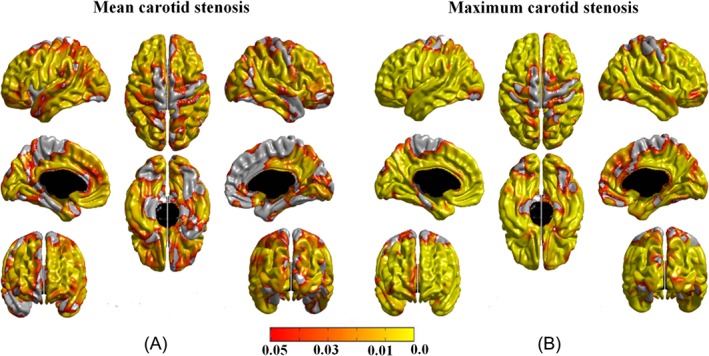
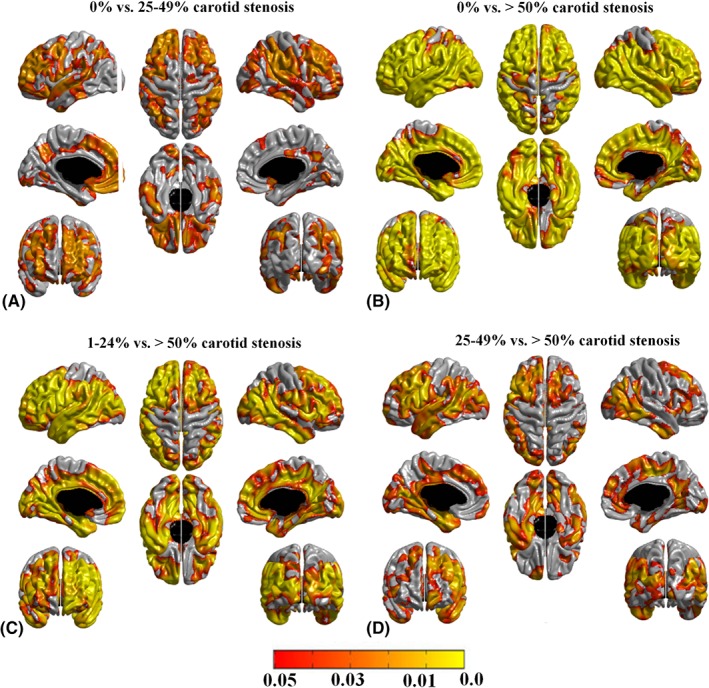
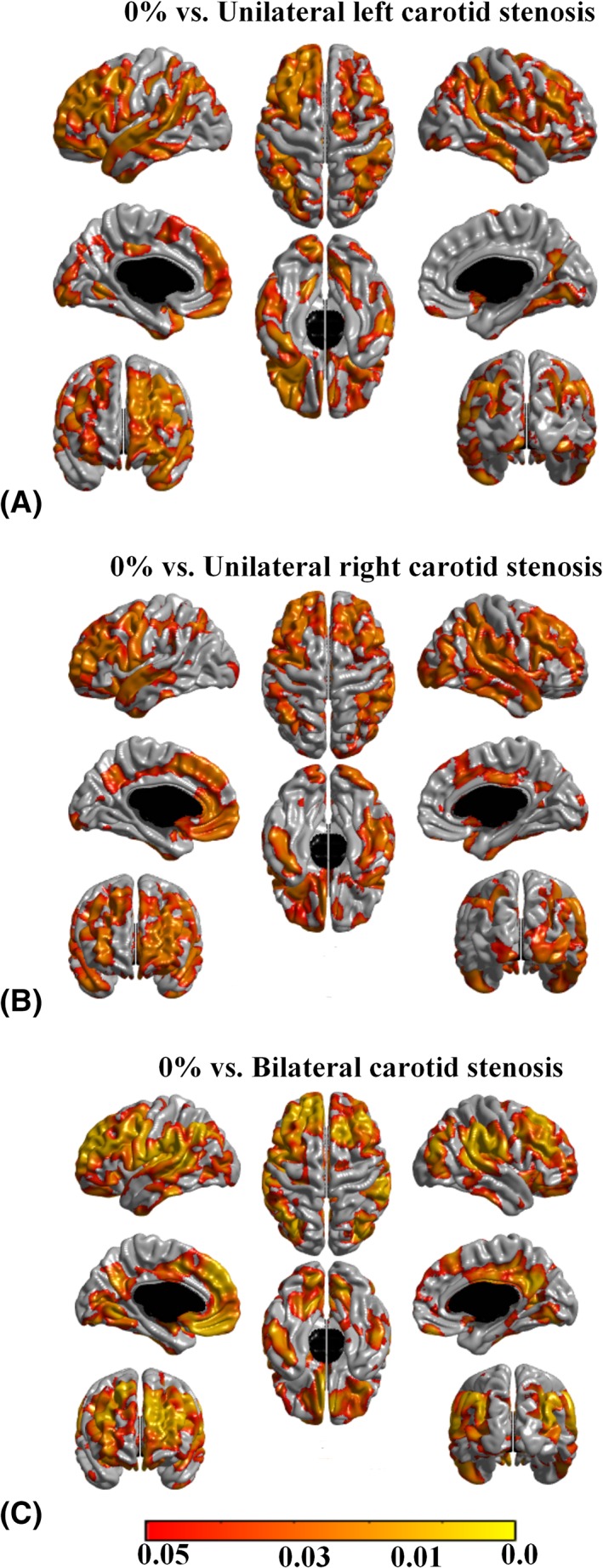
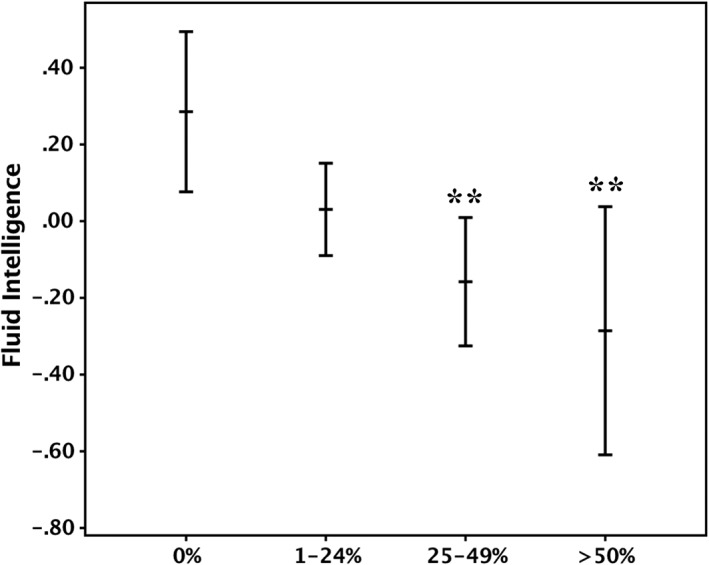
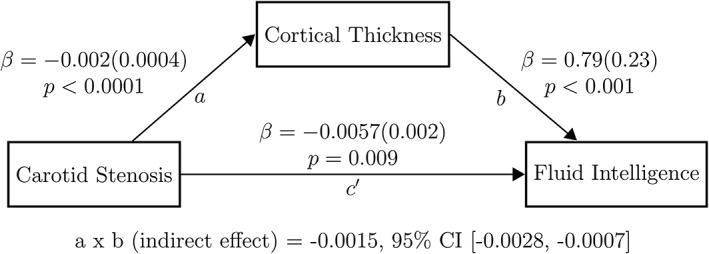
Results: A widespread negative association was identified between carotid stenosis (median = 15%) and cerebral cortical thickness at age 73 years, independent of the side of carotid stenosis, other carotid measures, VRFs, and IQ-11. This association increased in an almost dose-response relationship from mild to severe degrees of carotid stenosis, across the anterior and posterior circulation territories. A negative association was also noted between carotid stenosis and fluid intelligence (standardized beta coefficient = -0.151, p = 0.001), which appeared partly (approximately 22%) mediated by carotid stenosis-related thinning of the cerebral cortex.
Interpretation: The findings suggest that carotid stenosis represents a marker of processes that accelerate aging of the cerebral cortex and cognition that is in part independent of measurable VRFs. Cortical thinning within the anterior and posterior circulation territories partially mediated the relationship between carotid atheroma and fluid intelligence. Ann Neurol 2018;84:576-587.
© 2018 The Authors. Annals of Neurology published by Wiley Periodicals, Inc. on behalf of American Neurological Association.
Figures
References
-
- Tsivgoulis G, Vemmos K, Papamichael C, et al. Common carotid artery intima‐media thickness and the risk of stroke recurrence. Stroke 2006;37:1913–1916. - PubMed
-
- Muller M, Grobbee DE, Aleman A, et al. Cardiovascular disease and cognitive performance in middle‐aged and elderly men. Atherosclerosis 2007;190:143–149. - PubMed
-
- Bots ML, Breslau PJ, Briet E, et al. Cardiovascular determinants of carotid artery disease. The Rotterdam Elderly Study. Hypertension 1992;19:717–720. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
