

Worsening Knee Osteoarthritis Features on Magnetic Resonance Imaging 1 to 5 Years After Anterior Cruciate Ligament Reconstruction
- PMID: 30179520
- PMCID: PMC6379915
- DOI: 10.1177/0363546518789685
Worsening Knee Osteoarthritis Features on Magnetic Resonance Imaging 1 to 5 Years After Anterior Cruciate Ligament Reconstruction
Abstract
Background: An anterior cruciate ligament (ACL) injury is a well-established risk factor for the long-term development of radiographic osteoarthritis (OA). However, little is known about the early degenerative changes (ie, <5 years after injury) of individual joint features (ie, cartilage, bone marrow), which may be reversible and responsive to interventions.
Purpose: To describe early degenerative changes between 1 and 5 years after ACL reconstruction (ACLR) on magnetic resonance imaging (MRI) and explore participant characteristics associated with these changes.
Study design: Case-control study; Level of evidence, 3.
Methods: Seventy-eight participants (48 men; median age, 32 years; median body mass index [BMI], 26 kg/m2) underwent 3.0-T MRI at 1 and 5 years after primary hamstring autograft ACLR. Early tibiofemoral and patellofemoral OA features were assessed with the MRI Osteoarthritis Knee Score. The primary outcome was worsening (ie, incident or progressive) cartilage defects, bone marrow lesions (BMLs), osteophytes, and meniscal lesions. Logistic regression with generalized estimating equations evaluated participant characteristics associated with worsening features.
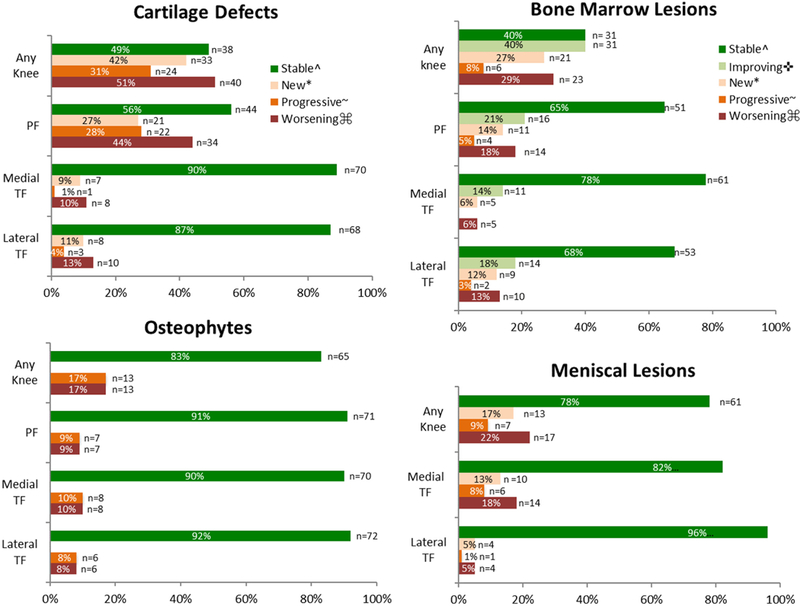
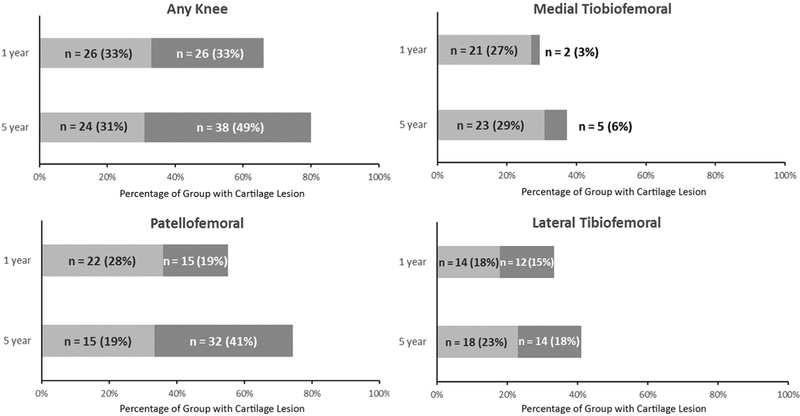
Results: Worsening of cartilage defects in any compartment occurred in 40 (51%) participants. Specifically, worsening in the patellofemoral and medial and lateral tibiofemoral compartments was present in 34 (44%), 8 (10%), and 10 (13%) participants, respectively. Worsening patellofemoral and medial and lateral tibiofemoral BMLs (14 [18%], 5 [6%], and 10 [13%], respectively) and osteophytes (7 [9%], 8 [10%], and 6 [8%], respectively) were less prevalent, while 17 (22%) displayed deteriorating meniscal lesions. Worsening of at least 1 MRI-detected OA feature, in either the patellofemoral or tibiofemoral compartment, occurred in 53 (68%) participants. Radiographic OA in any compartment was evident in 5 (6%) and 16 (21%) participants at 1 and 5 years, respectively. A high BMI (>25 kg/m2) was consistently associated with elevated odds (between 2- and 5-fold) of worsening patellofemoral and tibiofemoral OA features.
Conclusion: High rates of degenerative changes occur in the first 5 years after ACLR, particularly the development and progression of patellofemoral cartilage defects. Older patients with a higher BMI may be at particular risk and should be educated about this risk.
Keywords: anterior cruciate ligament; cartilage; knee; osteoarthritis.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: Support for this study was provided by Arthritis Australia (Grant in Aid), La Trobe University’s Sport, Exercise and Rehabilitation Research Focus Area (Project Grant), the Queensland Orthopaedic Physiotherapy Network (Project Grant), the University of Melbourne (Research Collaboration Grant), and the University of British Columbia’s Centre for Hip Health and Mobility (Society for Mobility and Health). B.E.P. is a recipient of a National Health and Medical Research Council (NHMRC) postgraduate scholarship (GNT 1114296). A.G.C.’s work was supported by an NHMRC Early Career Fellowship (Neil Hamilton Fairley Clinical Fellowship; GNT 1121173). The sponsors were not involved in the design and conduct of this study; in the analysis and interpretation of the data; and in the preparation, review, or approval of the article. A.G. is the president of Boston Imaging Core Lab and a consultant to Merck Serono, AstraZeneca, Pfizer, GE Healthcare, OrthoTrophix, Sanofi, and TissueGene.
Figures
References
-
- Altman RD, Gold GE. Atlas of individual radiographic features in osteoarthritis. Osteoarthritis Cartilage. 1995;(3)(suppl A):3–70. - PubMed
-
- Amin S, LaValley MP, Guermazi A, et al. The relationship between cartilage loss on magnetic resonance imaging and radiographic progression in men and women with knee osteoarthritis. Arthritis Rheum. 2005;52(10):3152–3159. - PubMed
-
- Anstey DE, Heyworth BE, Price MD, Gill TJ. Effect of timing of ACL reconstruction in surgery and development of meniscal and chondral lesions. Phys Sportsmed. 2012;40(1):36–40. - PubMed
-
- Ardern CL, Taylor NF, Feller JA, Webster KE. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br J Sports Med. 2014;48(21):1543–1552. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
