

Do Postoperative Results Differ in a Randomized Trial Between a Direct Anterior and a Direct Lateral Approach in THA?
- PMID: 30179928
- PMCID: PMC6345297
- DOI: 10.1097/CORR.0000000000000439
Do Postoperative Results Differ in a Randomized Trial Between a Direct Anterior and a Direct Lateral Approach in THA?
Abstract
Background: The direct lateral approach to THA provides good exposure and is associated with a low risk of dislocations, but can result in damage to the abductor muscles. The direct anterior approach does not incise muscle, and so recovery after surgery may be faster, but it has been associated with complications (including fractures and nerve injuries), and it involves a learning curve for surgeons who are unfamiliar with it. Few randomized trials have compared these approaches with respect to objective endpoints as well as validated outcome scores.
Questions/purposes: The purpose of this study was to compare the direct anterior approach with the direct lateral approach to THA with respect to (1) patient-reported and validated outcomes scores; (2) frequency and persistence of abductor weakness, as demonstrated by the Trendelenburg test; and (3) major complications such as infection, dislocation, reoperation, or neurovascular injury.
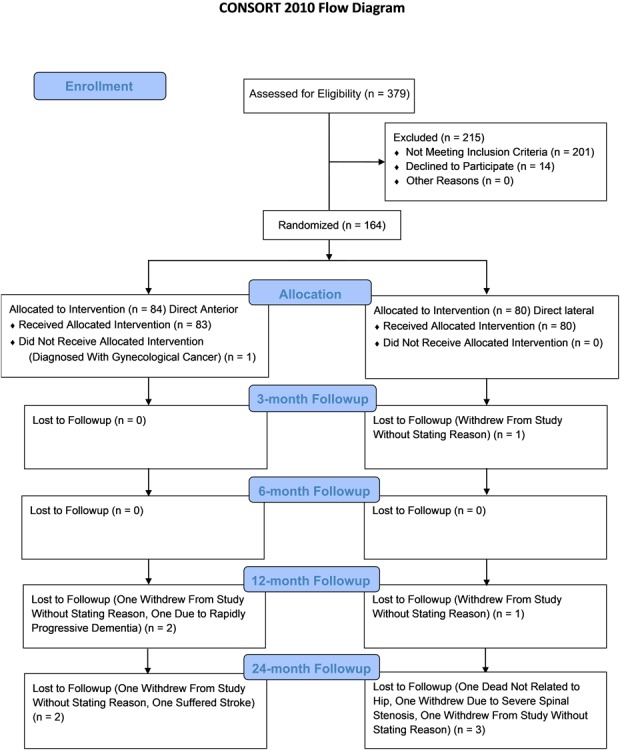
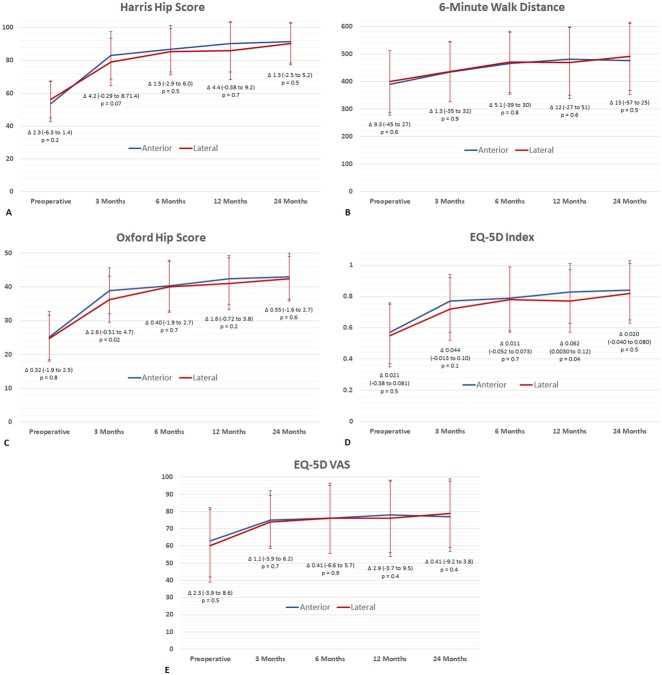
Methods: We performed a randomized controlled trial recruiting patients from January 2012 to June 2013. One hundred sixty-four patients with end-stage osteoarthritis were included and randomized to either the direct anterior or direct lateral approach. Before surgery and at 3, 6, 12, and 24 months, a physiotherapist recorded the Harris hip score (HHS), 6-minute walk distance (6MWD), and performed the Trendelenburg test directly after the 6MWD. The patients completed the Oxford Hip Score (OHS) and the EQ-5D. The groups were not different at baseline with respect to demographic data and preoperative scores. Both groups received the same pre- and postoperative regimes. Assessors were blinded to the approach used. One hundred fifty-four patients (94%) completed the 2-year followup; five patients from each group were lost to followup.
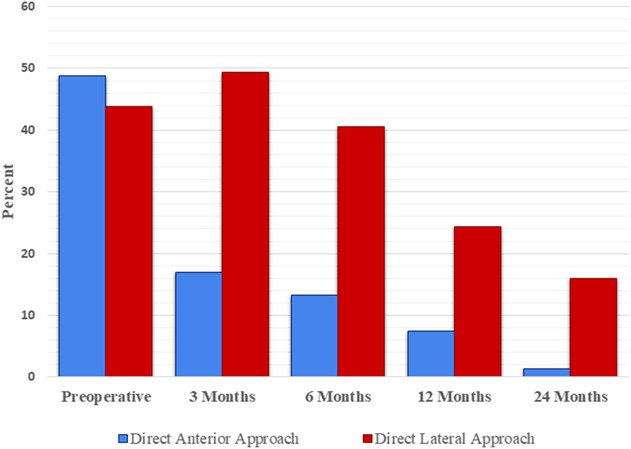
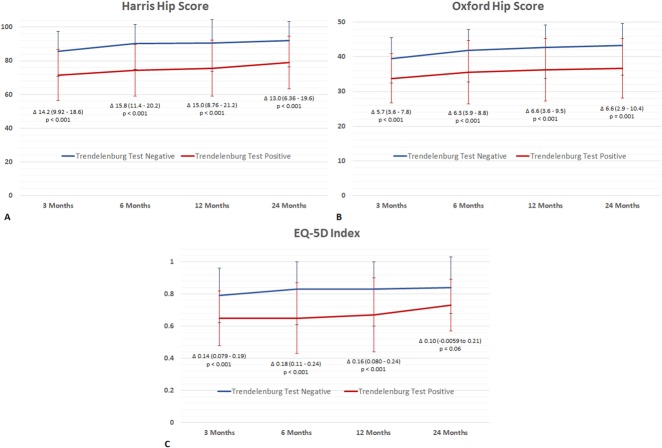
Results: There were few statistical differences and no clinically important differences in terms of validated or patient-reported outcomes scores (including the HHS, 6MWD, OHS, or EQ-5D) between the direct anterior and the lateral approach at any time point. A higher proportion of patients had a persistently positive Trendelenburg test 24 months after surgery in the lateral approach than the direct anterior approach (16% [12 of 75] versus 1% [one of 79]; odds ratio, 15; p = 0.001). Irrespective of approach, those with a positive Trendelenburg test had statistically and clinically important worse HHS, OHS, and EQ-5D scores than those with a negative Trendelenburg test. There were four major nerve injuries in the direct anterior group (three transient femoral nerve injuries, resolved by 3 months after surgery, and one tibial nerve injury with symptoms that persist 24 months after surgery) and none in the lateral approach.
Conclusions: Based on our findings, no case for superiority of one approach over the other can be made, except for the reduction in postoperative Trendelenburg test-positive patients using the direct anterior approach compared with when using the direct lateral approach. Irrespective of approach, patients with a positive Trendelenburg test had clinically worse scores than those with a negative test, indicating the importance of ensuring good abductor function when performing THA. The direct anterior approach was associated with nerve injuries that were not seen in the group treated with the lateral approach.
Level of evidence: Level I, therapeutic study.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: Do Postoperative Results Differ in a Randomized Trial Between a Direct Anterior and a Direct Lateral Approach in THA?Clin Orthop Relat Res. 2019 Jan;477(1):156-158. doi: 10.1097/CORR.0000000000000475. Clin Orthop Relat Res. 2019. PMID: 30575615 Free PMC article. No abstract available.
References
-
- Baker AS, Bitounis VC. Abductor function after total hip replacement. An electromyographic and clinical review. J Bone Joint Surg Br. 1989;71:47–50. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
