

Multivisceral IgG4-related disease presenting as recurrent massive gastrointestinal bleeding: a case report and literature review
- PMID: 30180812
- PMCID: PMC6123933
- DOI: 10.1186/s12876-018-0867-y
Multivisceral IgG4-related disease presenting as recurrent massive gastrointestinal bleeding: a case report and literature review
Abstract
Background: IgG4-related disease (IgG4-RD) is a newly recognized autoimmune systemic disorder characterized by elevated levels of serum IgG4 and abundant infiltration of IgG4-positive plasmacytes in the affected organs. The liver, biliary system and pancreas are the most commonly affected organs. However, involvement of the digestive tract is very rare. To date, only a few cases of isolated gastric IgG4-RD have been reported.
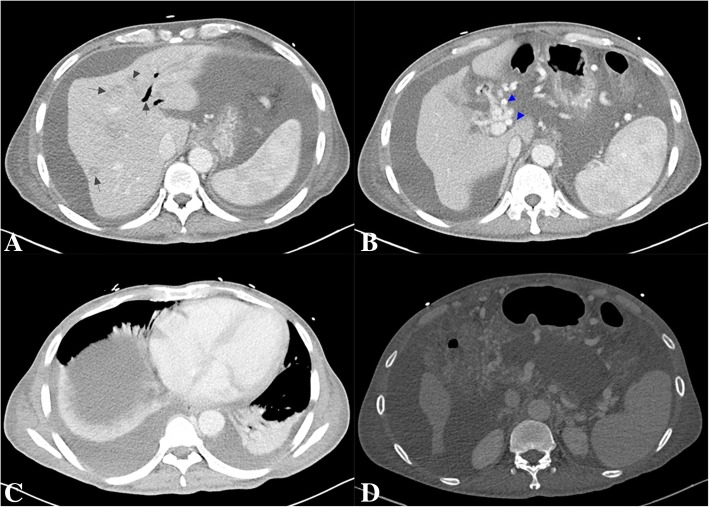
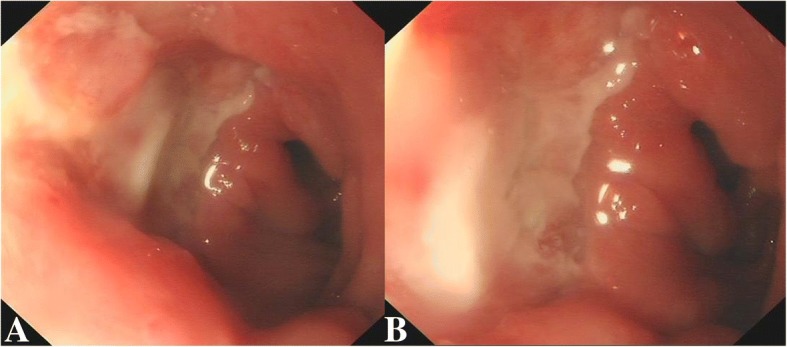
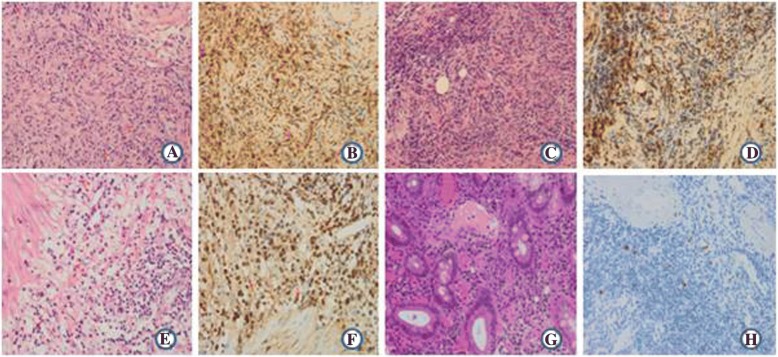
Case presentation: We present a case of IgG4-RD of the liver, gallbladder, pancreas and duodenum, which was clinically misinterpreted and thereafter over-treated. A 52-year-old male presented with obstructive jaundice for 3 years, melena for 5 months and hematemesis for 10 days. Three years prior, the patient had undergone biopsies of pancreatic lesions, liver lesions, cholecystectomy and choledochojejunostomy. Histopathology showed chronic inflammatory changes. Endoscopy at admission revealed a duodenal ulcer with active bleeding. Despite medical management, the patient presented with repeated gastrointestinal bleeding. Upon evaluation, serum IgG4 levels were found to be elevated. Histopathology of the duodenal ulcer biopsy and repeated examination of the gallbladder and pancreatic and liver biopsies confirmed IgG4 positive plasma cell infiltration. A definitive diagnosis of IgG4-RD was made and steroid administration was initiated. At last follow up, 11 months to-the-day after initiating steroid treatment, the patient was asymptomatic.
Conclusions: Notably, IgG4-RD of multiple digestive organs is still very rare. As a systemic disease, it is characterized by the infiltration of IgG4-bearing plasma cells and raised IgG4 levels. Histopathology findings remain the diagnostic gold standard for this disorder.
Keywords: Duodenal; Gallbladder; Gastrointestinal bleeding; IgG4-related disease; Liver; Pancreatic; Plasma cells.
Conflict of interest statement
Ethics approval and consent to participate
This article is a retrospective study and does not contain any studies with human subjects performed by any of the authors. So, the ethical approval was not necessary and West China Hospital of Sichuan University ethics committee can offer exempt ethical statement in support.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
[A case of duodenal ulcer as prominent manifestation of IgG4-related disease].Beijing Da Xue Xue Bao Yi Xue Ban. 2023 Dec 18;55(6):1125-1129. doi: 10.19723/j.issn.1671-167X.2023.06.026. Beijing Da Xue Xue Bao Yi Xue Ban. 2023. PMID: 38101799 Free PMC article. Chinese.
-
Skin lesions in a patient with IgG4-related disease.Clin Exp Dermatol. 2014 Aug;39(6):713-6. doi: 10.1111/ced.12372. Epub 2014 Jul 1. Clin Exp Dermatol. 2014. PMID: 24986022
-
[Clinical Practice and Examination for IgG4-Related Disease].Rinsho Byori. 2015 May;63(5):590-7. Rinsho Byori. 2015. PMID: 26524898 Review. Japanese.
-
IgG4-related disease involving vital organs diagnosed with lip biopsy: A case report and literature review.Medicine (Baltimore). 2016 Jun;95(24):e3970. doi: 10.1097/MD.0000000000003970. Medicine (Baltimore). 2016. PMID: 27311008 Free PMC article. Review.
-
Histopathology of IgG4-Related Autoimmune Hepatitis and IgG4-Related Hepatopathy in IgG4-Related Disease.Semin Liver Dis. 2016 Aug;36(3):229-41. doi: 10.1055/s-0036-1584320. Epub 2016 Jul 28. Semin Liver Dis. 2016. PMID: 27466793
Cited by
-
IgG4-Related Oesophageal Disease with Cytomegalovirus Infection: A Case Report.J Pers Med. 2023 Mar 9;13(3):493. doi: 10.3390/jpm13030493. J Pers Med. 2023. PMID: 36983676 Free PMC article.
-
Curable giant hematoma due to small bowel mesenteric laceration after screening colonoscopy: a case report.Ann Med Surg (Lond). 2025 Jan 9;87(1):326-330. doi: 10.1097/MS9.0000000000002739. eCollection 2025 Jan. Ann Med Surg (Lond). 2025. PMID: 40109587 Free PMC article.
-
Cytopenias in Autoimmune Liver Diseases-A Review.J Clin Med. 2025 Mar 4;14(5):1732. doi: 10.3390/jcm14051732. J Clin Med. 2025. PMID: 40095848 Free PMC article. Review.
References
-
- Zhang W, Xue F, Liu MC, et al. 36 cases IgG4 related clinical analysis. [Chinese] Chinese. Journal of Nephrology. 2016;32:253–258.
-
- Li YM, Wang H, Fang F, et al. IgG4 related clinical feature analysis. [Chinese] National Medical Journal of China. 2015;95:3281–3284. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
