

The OptimaMed intervention to reduce inappropriate medications in nursing home residents with severe dementia: results from a quasi-experimental feasibility pilot study
- PMID: 30180821
- PMCID: PMC6123948
- DOI: 10.1186/s12877-018-0895-z
The OptimaMed intervention to reduce inappropriate medications in nursing home residents with severe dementia: results from a quasi-experimental feasibility pilot study
Abstract
Background: Medication regimens in nursing home (NH) residents with severe dementia should be frequently reviewed to avoid inappropriate medication, overtreatment and adverse drug events, within a comfort care approach. This study aimed at testing the feasibility of an interdisciplinary knowledge exchange (KE) intervention using a medication review guidance tool categorizing medications as either "generally", "sometimes" or "exceptionally" appropriate for NH residents with severe dementia.
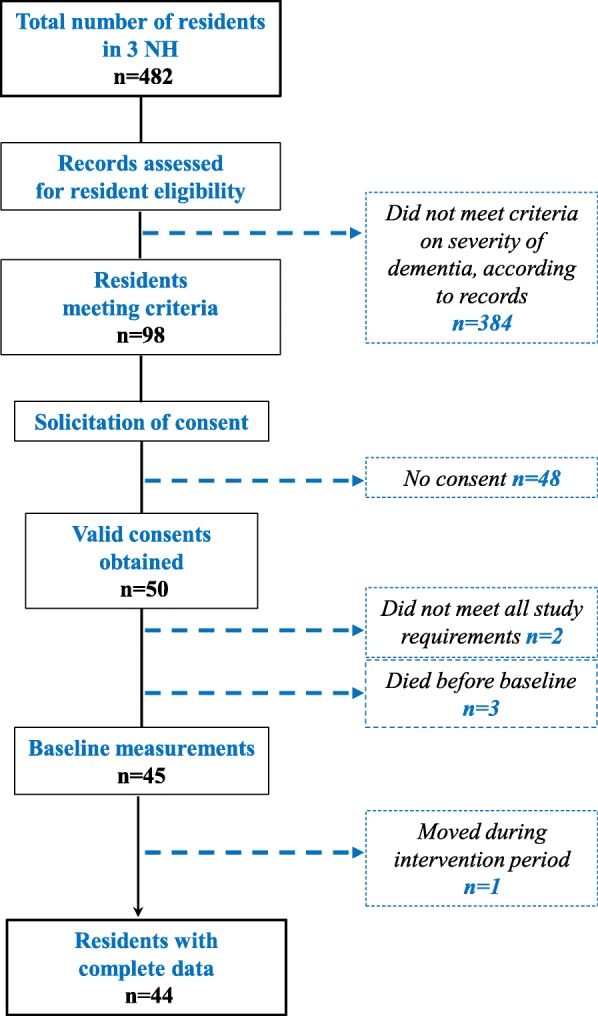
Methods: A quasi-experimental feasibility pilot study with 44 participating residents aged 65 years or over with severe dementia was carried out in three NH in Quebec City, Canada. The intervention comprised an information leaflet for residents' families, a 90-min KE session for NH general practitioners (GP), pharmacists and nurses focusing on the medication review guidance tool, a medication review by the pharmacists for participating residents with ensuing team discussion on medication changes, and a post-intervention KE session to obtain feedback from team staff. Medication regimens and levels of pain and of agitation of the participants were evaluated at baseline and at 4 months post-intervention. A questionnaire for team staff explored perceived barriers and facilitators. Statistical differences in measures comparing pre and post-intervention were assessed using paired t-tests and Cochran's-Q tests.
Results: The KE sessions reached 34 NH team staff (5 GP, 4 pharmacists, 6 heads of care unit and 19 staff nurses). Forty-four residents participated in the study and were followed for a mean of 104 days. The total number of regular medications was 372 pre and 327 post-intervention. The mean number of regular medications per resident was 7.86 pre and 6.81 post-intervention. The odds ratios estimating the risks of using any regular medication or a "sometimes appropriate" medication post-intervention were 0.81 (95% CI: 0.71-0.92) and 0.83 (95% CI: 0.74-0.94), respectively.
Conclusion: A simple KE intervention using a medication review guidance tool categorizing medications as being either "generally", "sometimes" or "exceptionally" appropriate in severe dementia was well received and accompanied by an overall reduction in medication use by NH residents with severe dementia. Levels of agitation were unaffected and there was no clinically significant changes in levels of pain. Staff feedback provided opportunities to improve the intervention.
Keywords: Dementia; Inappropriate medication use; Intervention; Long-term care.
Conflict of interest statement
Ethics approval and consent to participate
The present study was proposed to the local Health and Social Services Board (HSSB), which suggested the name of three NHs that agreed to participate. The study was approved by the HSSB and the
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
None of the financing or supporting institutions had any influence on the study’s objective, design, results or conclusion.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
