

Discovery of the IL-23/IL-17 Signaling Pathway and the Treatment of Psoriasis
- PMID: 30181299
- PMCID: PMC6129988
- DOI: 10.4049/jimmunol.1800013
Discovery of the IL-23/IL-17 Signaling Pathway and the Treatment of Psoriasis
Abstract
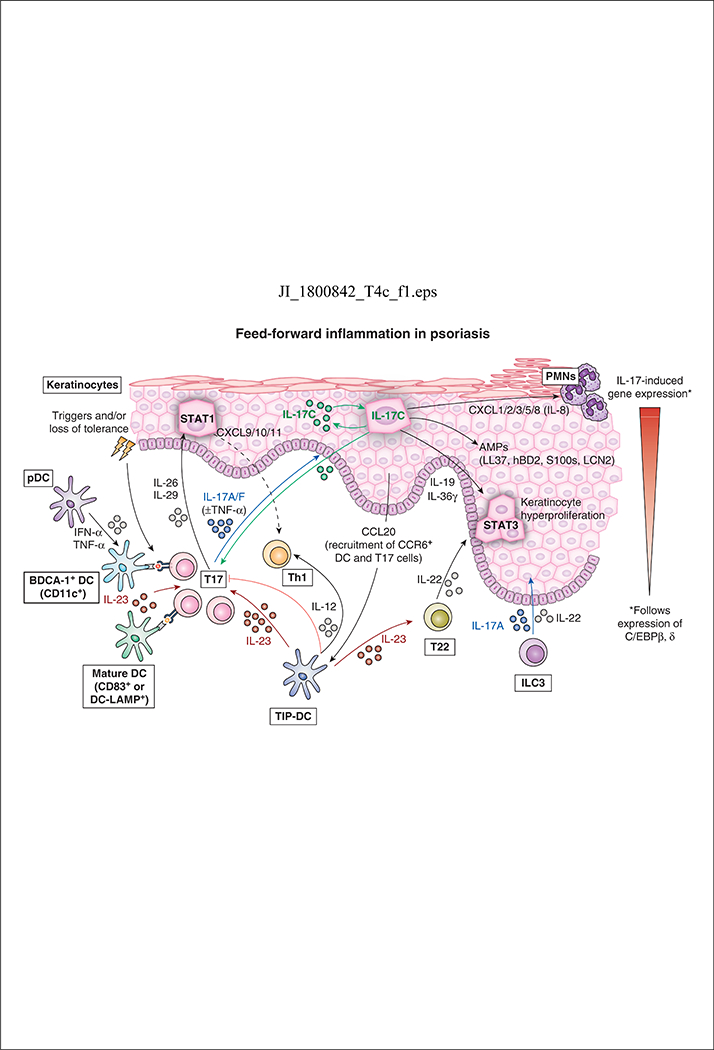
Psoriasis vulgaris is a common, heterogeneous, chronic inflammatory skin disease characterized by thickened, red, scaly plaques and systemic inflammation. Psoriasis is also associated with multiple comorbid conditions, such as joint destruction, cardiovascular disease, stroke, hypertension, metabolic syndrome, and chronic kidney disease. The discovery of IL-17-producing T cells in a mouse model of autoimmunity transformed our understanding of inflammation driven by T lymphocytes and associations with human inflammatory diseases, such as psoriasis. Under the regulation of IL-23, T cells that produce high levels of IL-17 create a self-amplifying, feed-forward inflammatory response in keratinocytes that drives the development of thickened skin lesions infiltrated with a mixture of inflammatory cell populations. Recently, the Food and Drug Administration approved multiple highly effective psoriasis therapies that disrupt IL-17 (secukinumab, ixekizumab, and brodalumab) and IL-23 (guselkumab and tildrakizumab) signaling in the skin, thus leading to a major paradigm shift in the way that psoriatic disease is managed.
Copyright © 2018 by The American Association of Immunologists, Inc.
Figures
References
-
- Rachakonda TD, Schupp CW, and Armstrong AW. 2014. Psoriasis prevalence among adults in the United States. J Am Acad Dermatol 70: 512–516. - PubMed
-
- Gelfand JM, Troxel AB, Lewis JD, Kurd SK, Shin DB, Wang X, Margolis DJ, and Strom BL. 2007. The risk of mortality in patients with psoriasis: results from a population-based study. Arch Dermatol 143: 1493–1499. - PubMed
-
- Gottlieb SL, Gilleaudeau P, Johnson R, Estes L, Woodworth TG, Gottlieb AB, and Krueger JG. 1995. Response of psoriasis to a lymphocyte-selective toxin (DAB389IL-2) suggests a primary immune, but not keratinocyte, pathogenic basis. Nat Med 1: 442–447. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
