

The Effect of Alginate in Gastroesophageal Reflux in Infants
- PMID: 30182358
- PMCID: PMC6267531
- DOI: 10.1007/s40272-018-0314-0
The Effect of Alginate in Gastroesophageal Reflux in Infants
Abstract
Background: Guidelines are contradictory regarding the use of alginate in infants with persisting gastroesophageal reflux (GER). While The British National Institute for Health and Care (NICE) guidelines consider alginate as a treatment option, the guidelines of the European and North-American Societies for Pediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN, NASPGHAN) do not recommend alginates.
Aims: We assessed the efficacy of alginate to reduce GER episodes in infants.
Methods: In a prospective, observational study, we consecutively enrolled all infants referred for pH-multiple intraluminal impedance (pH-MII) recording because of persisting GER symptoms not responsive to behavior and dietetic modifications. A 48-h pH-MII was performed in all infants; a baseline recording was performed during the first 24 h while magnesium or sodium alginate was administered during the second 24 h. The primary endpoint was the difference in the total number of GER episodes per 24 h between the baseline day and the second day during which the alginate was administered. The secondary outcome was the difference in symptoms between each period. We also compared other pH-MII data from before and during alginate administration.
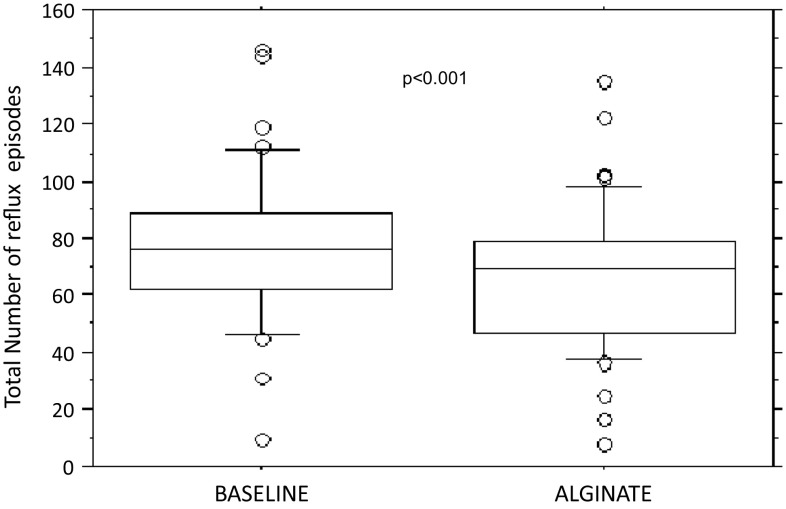
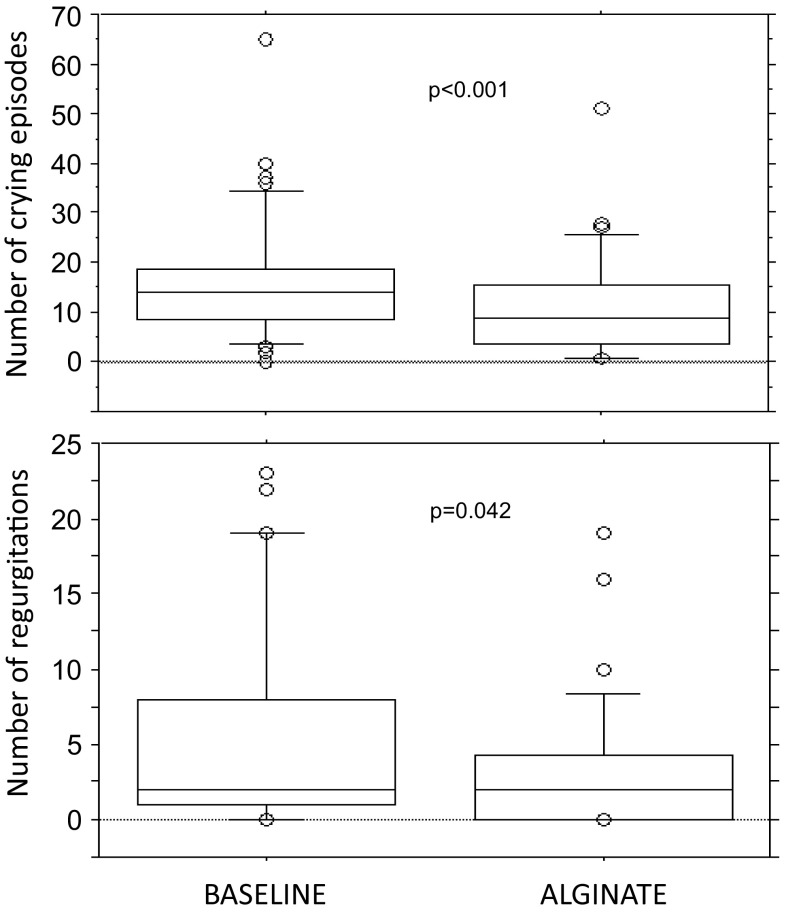
Results: We recruited 43 infants (median age 68 days, range 25-306); three pH-MII tracings were excluded because of artifacts. The median number of all MII reflux episodes was significantly reduced during alginate administration (76.0 vs 69.5; p < 0.001). Crying-fussiness, cough and regurgitation episodes all significantly improved during alginate administration (p = 0.00012; p = 0.005 and p = 0.04, respectively). The following MII parameters also decreased during the alginate administration: acid (19.0 vs 14.5; p < 0.04), non-acid (52.0 vs 49.5; p < 0.004), proximal GER episodes (46.0 vs 41.4; p < 0.007), and bolus exposure index (1.9 vs 1.6; p = 0.002). At least three out of seven pH-MII parameters decreased by > 10% during the alginate period in 31/40 infants (77.5%), without a significant difference between magnesium and sodium alginate.
Conclusion: These results suggest that alginate significantly decreases the number and extension of both acid and non-acid reflux episodes and associated symptoms in infants.
Conflict of interest statement
SS has participated as a consultant and/or speaker for Danone-Nutricia, Deca, IMS-Health, Menarini, and Nestle. YV has participated as a clinical investigator, and/or advisory board member, and/or consultant, and/or speaker for Abbott Nutrition, Biocodex, Danone, Nestle Health Science, Nestle Nutrition Institute, Nutricia, Mead Johnson, and United Pharmaceuticals. None of the above manufacturers and companies have had any input or involvement in any aspect of this study. The other authors have no conflicts of interest to disclose.
Figures
References
-
- Rosen R, Vandenplas Y, Singendonk M, et al. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the north american society for pediatric gastroenterology, hepatology, and nutrition and the European society for pediatric gastroenterology, hepatology, and nutrition. J Pediatr Gastroenterol Nutr. 2018;66(3):516–554. doi: 10.1097/MPG.0000000000001889. - DOI - PMC - PubMed
-
- National Institute for Health and Care Excellence (NICE). Gastro-oesophageal reflux disease: recognition, diagnosis and management in children and young people. (Clinical Guideline 193) 2015. http://www.nice.org.uk/guidance/NG1. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
