

Time spent at blood pressure target and the risk of death and cardiovascular diseases
- PMID: 30183734
- PMCID: PMC6124703
- DOI: 10.1371/journal.pone.0202359
Time spent at blood pressure target and the risk of death and cardiovascular diseases
Abstract
Background: The time a patient spends with blood pressure at target level is an intuitive measure of successful BP management, but population studies on its effectiveness are as yet unavailable.
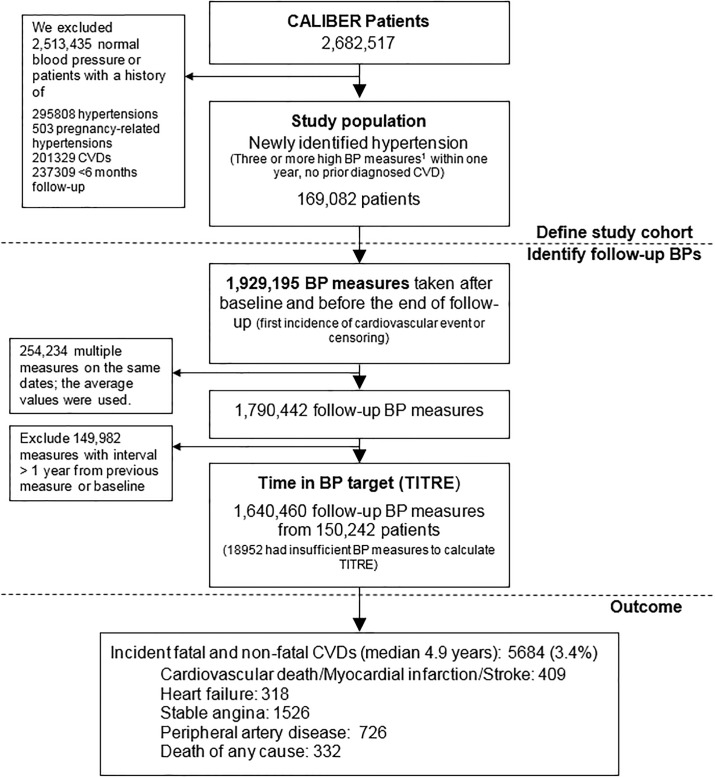
Method: We identified a population-based cohort of 169,082 individuals with newly identified high blood pressure who were free of cardiovascular disease from January 1997 to March 2010. We used 1.64 million clinical blood pressure readings to calculate the TIme at TaRgEt (TITRE) based on current target blood pressure levels.
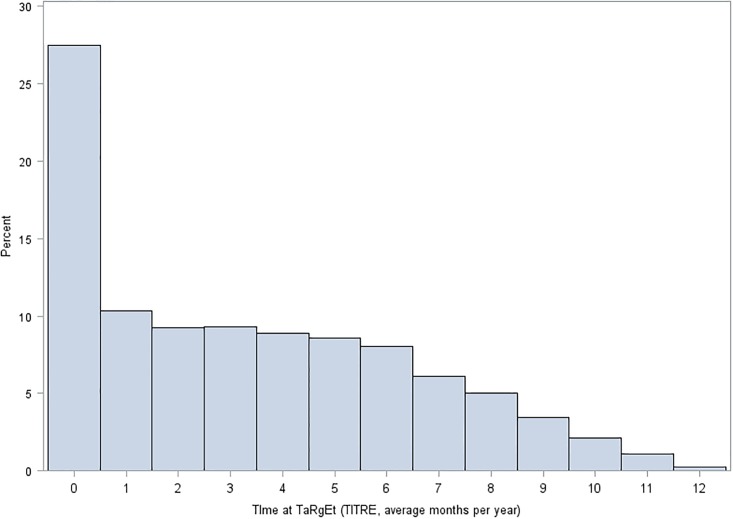
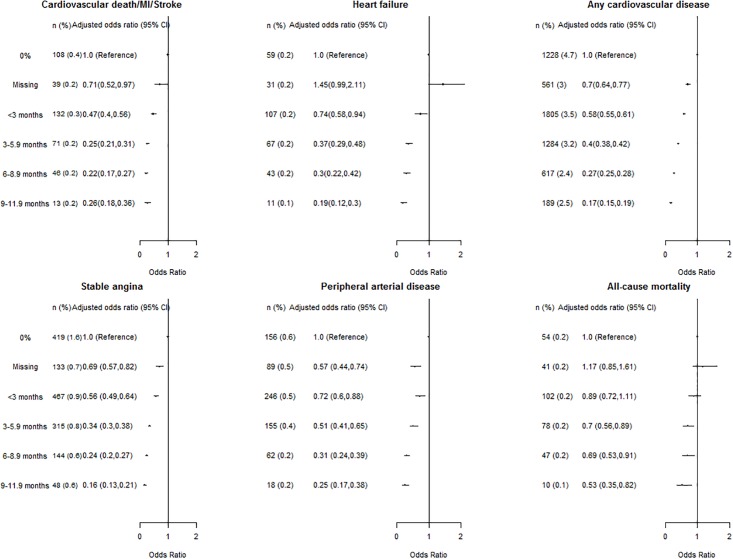
Result: The median (Inter-quartile range) TITRE among all patients was 2.8 (0.3, 5.6) months per year, only 1077 (0.6%) patients had a TITRE ≥11 months. Compared to people with a 0% TITRE, patients with a TITRE of 3-5.9 months, and 6-8.9 months had 75% and 78% lower odds of the composite of cardiovascular death, myocardial infarction and stroke (adjusted odds ratios, 0.25 (95% confidence interval: 0.21, 0.31) and 0.22 (0.17, 0.27), respectively). These associations were consistent for heart failure and any cardiovascular disease and death (comparing a 3-5.9 month to 0% TITRE, 63% and 60% lower in odds, respectively), among people who did or did not have blood pressure 'controlled' on a single occasion during the first year of follow-up, and across groups defined by number of follow-up BP measure categories.
Conclusion: Based on the current frequency of measurement of blood pressure this study suggests that few newly hypertensive patients sustained a complete, year-round on target blood pressure over time. The inverse associations between a higher TITRE and lower risk of incident cardiovascular diseases were independent of widely-used blood pressure 'control' indicators. Randomized trials are required to evaluate interventions to increase a person's time spent at blood pressure target.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Rapsomaniki E, Timmis A, George J, Pujades-Rodriguez M, Shah AD, Denaxas S, et al. (2014) Blood pressure and incidence of twelve cardiovascular diseases: lifetime risks, healthy life-years lost, and age-specific associations in 1.25 million people. Lancet 383: 1899–1911. 10.1016/S0140-6736(14)60685-1 - DOI - PMC - PubMed
-
- Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Bohm M, et al. (2013) 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 34: 2159–2219. 10.1093/eurheartj/eht151 - DOI - PubMed
-
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018. May 15;71(19):e127–e248. 10.1016/j.jacc.2017.11.006 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
