

Integrating Facility-Based Surveillance With Healthcare Utilization Surveys to Estimate Enteric Fever Incidence: Methods and Challenges
- PMID: 30184162
- PMCID: PMC6226762
- DOI: 10.1093/infdis/jiy494
Integrating Facility-Based Surveillance With Healthcare Utilization Surveys to Estimate Enteric Fever Incidence: Methods and Challenges
Abstract
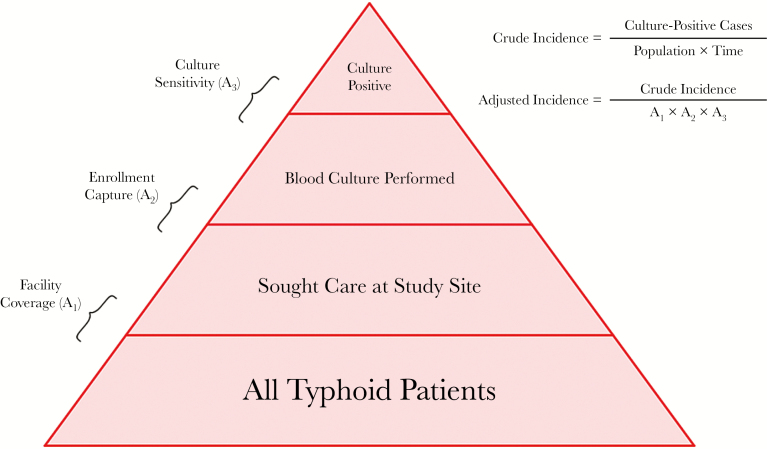
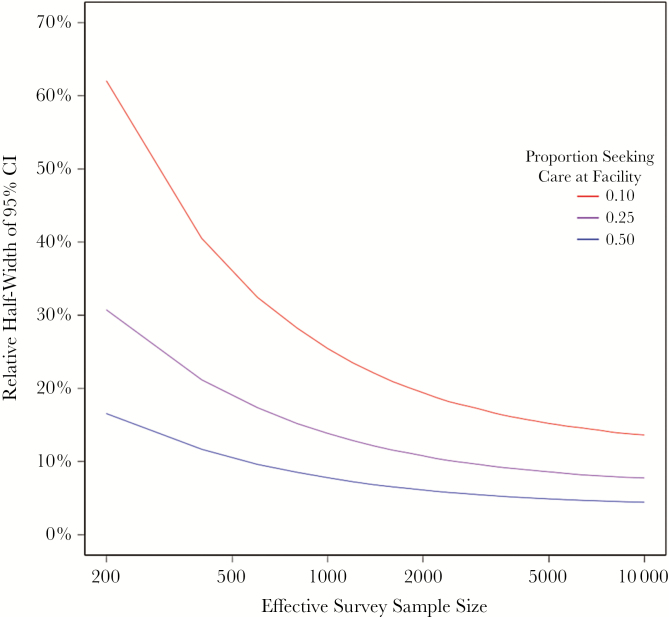
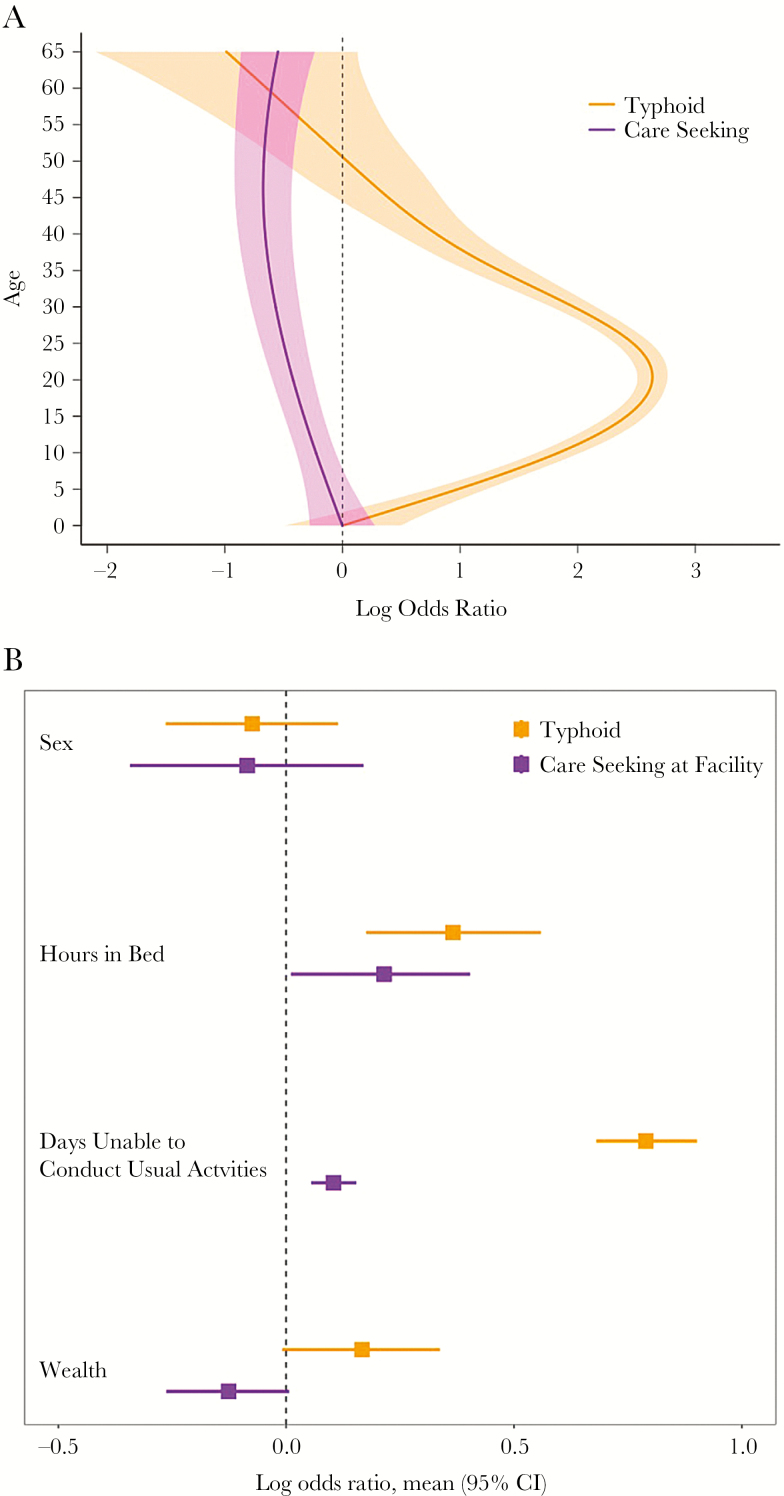
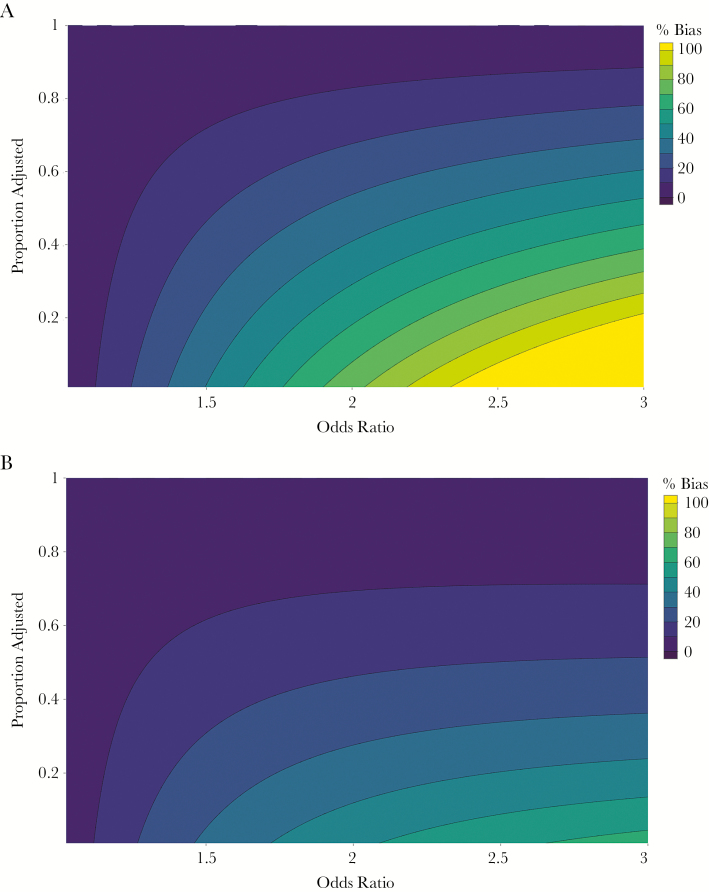
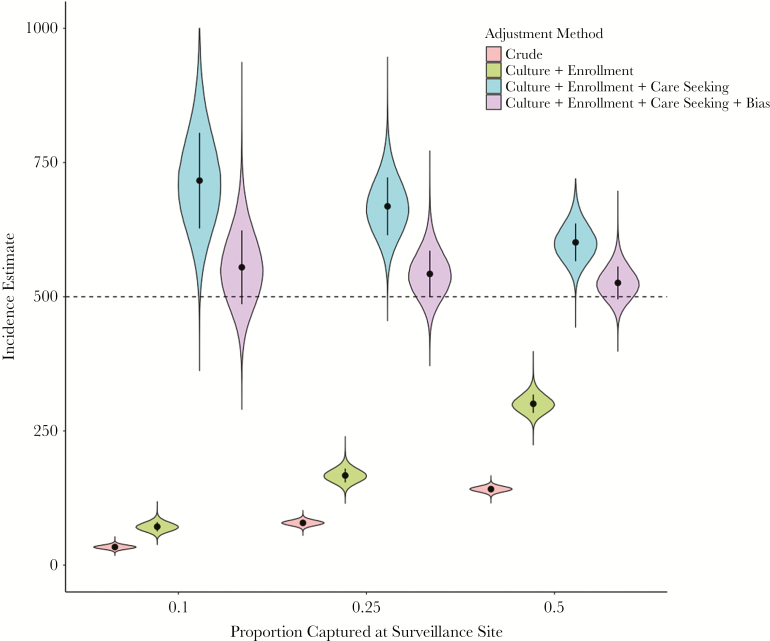
Cohort studies and facility-based sentinel surveillance are common approaches to characterizing infectious disease burden, but present trade-offs; cohort studies are resource-intensive and may alter disease natural history, while sentinel surveillance underestimates incidence in the population. Hybrid surveillance, whereby facility-based surveillance is paired with a community-based healthcare utilization assessment, represents an alternative approach to generating population-based disease incidence estimates with moderate resource investments. Here, we discuss this method in the context of the Surveillance for Enteric Fever in Asia Project (SEAP) study. We describe how data are collected and utilized to adjust enteric fever incidence for blood culture sensitivity, facility-based enrollment, and healthcare seeking, incorporating uncertainty in these parameters in the uncertainty around incidence estimates. We illustrate how selection of surveillance sites and their coverage may influence precision and bias, and we identify approaches in the study design and analysis to minimize and control for these biases. Rigorously designed hybrid surveillance systems can be an efficient approach to generating population-based incidence estimates for infectious diseases.
Figures
References
-
- Mogasale V, Maskery B, Ochiai RL, et al. . Burden of typhoid fever in low-income and middle-income countries: a systematic, literature-based update with risk-factor adjustment. Lancet Glob Health 2014; 2:e570–80. - PubMed
-
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017; 390(10100): P1211–1259. doi:10.1016/S0140-6736(17)32154-2 - PMC - PubMed
-
- World Health Organization. Typhoid vaccines: WHO position paper—March 2018. WHO Wkly Epidemiol Rec. 2018; 93:153–72.
-
- Sinha A, Sazawal S, Kumar R, et al. . Typhoid fever in children aged less than 5 years. Lancet 1999; 354:734–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
