

Arterial blood gas changes during cardiac arrest and cardiopulmonary resuscitation combined with passive oxygenation/ventilation: a METI HPS study
- PMID: 30185100
- PMCID: PMC6259407
- DOI: 10.1177/0300060518786916
Arterial blood gas changes during cardiac arrest and cardiopulmonary resuscitation combined with passive oxygenation/ventilation: a METI HPS study
Abstract
Objective: High-fidelity simulators can simulate physiological responses to medical interventions. The dynamics of the partial arterial pressure of oxygen (PaO2), partial arterial pressure of carbon dioxide (PaCO2), and oxygen pulse saturation (SpO2) during simulated cardiopulmonary resuscitation (CPR) were observed and compared with the results from the literature.
Methods: Three periods of cardiac arrest were simulated using the METI Human Patient Simulator™ (Medical Education Technologies, Inc., Sarasota, FL, USA): cardiac arrest, chest compression-only CPR, and chest compression-only CPR with continuous flow insufflation of oxygen (CFIO).
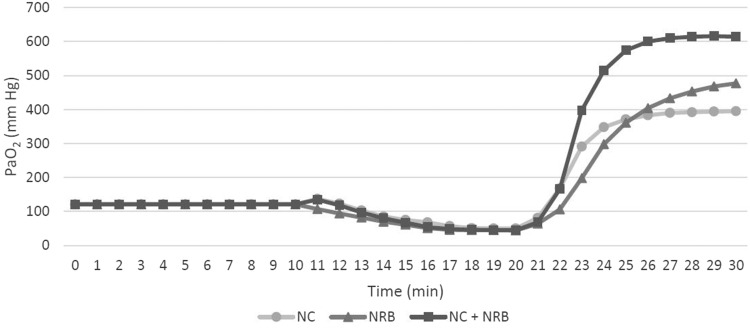
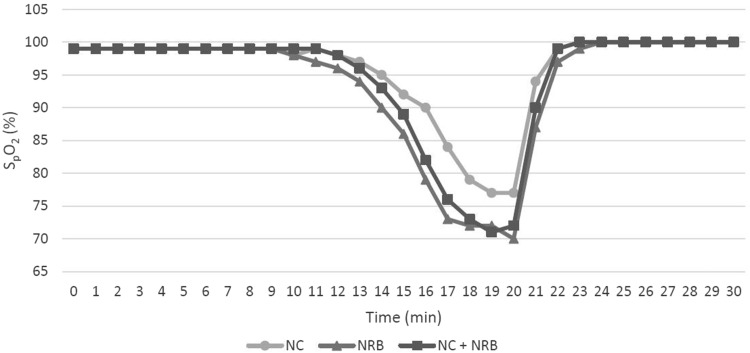
Results: In the first period, the observed values remained constant. In the second period, PaCO2 started to rise and peaked at 63.5 mmHg. In the CFIO period, PaCO2 slightly fell. PaO2 and SpO2 declined only in the second period, reaching their lowest values of 44 mmHg and 70%, respectively. In the CFIO period, PaO2 began to rise and peaked at 614 mmHg. SpO2 exceeded 94% after 2 minutes of CFIO.
Conclusions: The METI Human Patient Simulator™ accurately simulated the dynamics of changes in PaCO2. Use of this METI oxygenation model has some limitations because the simulated levels of PaO2 and SpO2 during cardiac arrest correlate poorly with the results from published studies.
Keywords: Patient-specific modeling; blood gas analysis; cardiac arrest; cardiopulmonary resuscitation; high-fidelity simulator; pulmonary ventilation.
Figures

Similar articles
-
[Effects of interposed abdominal pulling-pressing cardiopulmonary resuscitation on hemodynamics and oxygen metabolism in patients with cardiac arrest].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019 Nov;31(11):1406-1410. doi: 10.3760/cma.j.issn.2095-4352.2019.11.018. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019. PMID: 31898574 Chinese.
-
[Effects of active abdominal compression-decompression CPR on oxygen metabolism and prognosis in patients with cardiac arrest].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017 Dec;29(12):1117-1121. doi: 10.3760/cma.j.issn.2095-4352.2017.12.013. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017. PMID: 29216947 Clinical Trial. Chinese.
-
[Interposed abdominal pulling-pressing cardiopulmonary resuscitation improve the resuscitation effect for patients with cardiac arrest].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018 May;30(5):466-470. doi: 10.3760/cma.j.issn.2095-4352.2018.05.014. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018. PMID: 29764553 Chinese.
-
[Ventilation during cardiopulmonary resuscitation (CPR). A literature study and analysis of ventilation strategies].Anaesthesist. 1997 Feb;46(2):133-41. doi: 10.1007/s001010050383. Anaesthesist. 1997. PMID: 9133175 Review. German.
-
Reassessing the need for ventilation during CPR.Ann Emerg Med. 1996 May;27(5):569-75. doi: 10.1016/s0196-0644(96)70159-2. Ann Emerg Med. 1996. PMID: 8629777 Review.
Cited by
-
Factors affecting the return of spontaneous circulation in cardiac arrest patients.Medicine (Baltimore). 2024 Dec 27;103(52):e40966. doi: 10.1097/MD.0000000000040966. Medicine (Baltimore). 2024. PMID: 39969385 Free PMC article.
References
-
- Perkins GD, Handley AJ, Koster RW, et al. European resuscitation council guidelines for resuscitation 2015 Section 2. Adult basic life support and automated external defibrillation. Resuscitation 2015; 95: 81–99. - PubMed
-
- Idris AH. Reassessing the need for ventilation during CPR. Ann Emerg Med 1996; 27: 569–575. - PubMed
-
- Aufderheide TP, Sigurdsson G, Pirrallo RG, et al. Hyperventilation-induced hypotension during cardiopulmonary resuscitation. Circulation 2004; 109: 1960–1965. - PubMed
-
- Aufderheide TP, Lurie KG. Death by hyperventilation: a common and life-threatening problem during cardiopulmonary resuscitation. Crit Care Med 2004; 32: S345–S351. - PubMed
-
- Locke CJ, Berg RA, Sanders AB, et al. Bystander cardiopulmonary resuscitation. Concerns about mouth-to-mouth contact. Arch Intern Med 1995; 155: 938–943. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
