

Understanding the persistence of vertical (stand-alone) HIV clinics in the health system in Uganda: a qualitative synthesis of patient and provider perspectives
- PMID: 30185191
- PMCID: PMC6126041
- DOI: 10.1186/s12913-018-3500-4
Understanding the persistence of vertical (stand-alone) HIV clinics in the health system in Uganda: a qualitative synthesis of patient and provider perspectives
Abstract
Background: Although there is mounting evidence and policy guidance urging the integration of HIV services into general health systems in countries with a high HIV burden, vertical (stand-alone) HIV clinics are still common in Uganda. We sought to describe the specific contexts underpinning the endurance of vertical HIV clinics in Uganda.
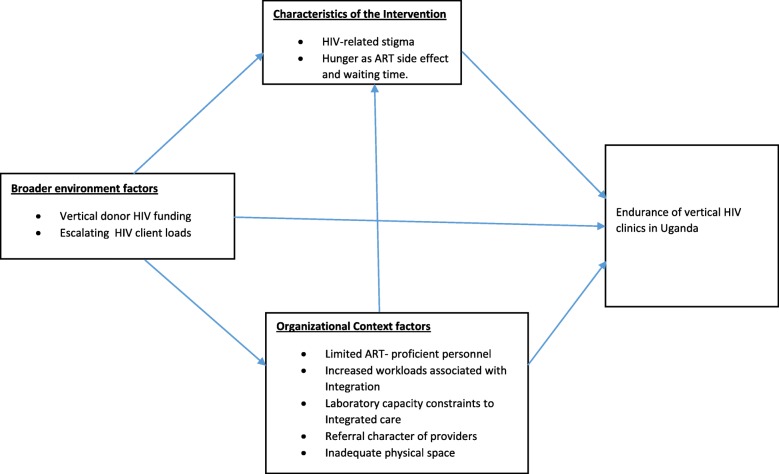
Methods: A qualitative research design was adopted. Semi-structured interviews were conducted with the heads of HIV clinics, clinicians and facility in-charges (n = 78), coupled with eight focus group discussions (64 participants) with patients from 16 health facilities purposively selected, from a nationally-representative sample of 195 health facilities across Uganda, because they run stand-alone HIV clinics. Data were analyzed by thematic approach as guided by the theory proposed by Shediac-Rizkallah & Bone (1998) which identifies; Intervention characteristics, organizational context, and broader environment factors as potentially influential on health programme sustainability.
Results: Intervention characteristics: Provider stigma was reported to have been widespread in the integrated care experience of participating health facilities which necessitated the establishment of stand-alone HIV clinics. HIV disease management was described as highly specialized which necessitated a dedicated workforce and vertical HIV infrastructure such as counselling rooms. Organizational context: Participating health facilities reported health-system capacity constraints in implementing integrated systems of care due to a shortage of ART-proficient personnel and physical space, a lack of laboratory capacity to concurrently conduct HIV and non-HIV tests and increased workloads associated with implementing integrated care. Broader environment factors: Escalating HIV client loads and external HIV funding architectures were perceived to have perpetuated verticalized HIV programming over the past decade.
Conclusion: Our study offers in-depth, contextualized insights into the factors contributing to the endurance of vertical HIV clinics in Uganda. Our analysis suggests that there is a complex interaction in supply-side constraints (shortage of ART-proficient personnel, increased workloads, laboratory capacity deficiencies) and demand-side factors (escalating demand for HIV services, psychosocial barriers to HIV care) as well as the specialized nature of HIV disease management which pose challenges to the integrated-health services agenda.
Keywords: Antiretroviral therapy; Global health initiatives; HIV; Health systems; Implementation research; Integration; Service delivery.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval was granted by Makerere University, School of Public Health, Institutional Review Board. Permission to conduct research was granted by The Uganda National Council of Science and Technology (UNCST) under instrument: No.HS1512. All interview participants signed a written informed consent form before participating in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- WHO. Operations Manual for Delivery of HIV Prevention, Care and treatment at primary health Centres in high-prevalence, Resource-Constrained Settings Edition 1.2008. www.who.int/hiv/pub/imai/operations_manual/en/. - PubMed
-
- Odeny TA, Penner J, Lewis-Kulzer J, Leslie HH, Shade SB, Adero W, Kioko J, Cohen CR, Bukusi EA. Integration of HIV care with primary health care services: effect on patient satisfaction and stigma in rural Kenya. AIDS Res Treat. 2013;2013. https://www.hindawi.com/journals/art/2013/485715/. - PMC - PubMed
-
- Smit JA, Church K, Milford C, Harrison AD, Beksinska ME. Key informant perspectives on policy-and service-level challenges and opportunities for delivering integrated sexual and reproductive health and HIV care in South Africa. BMC Health Serv Res. 2012;12(1):48. doi: 10.1186/1472-6963-12-48. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
