

Association of guideline and policy changes with incidence of lifestyle advice and treatment for uncomplicated mild hypertension in primary care: a longitudinal cohort study in the Clinical Practice Research Datalink
- PMID: 30185571
- PMCID: PMC6129091
- DOI: 10.1136/bmjopen-2018-021827
Association of guideline and policy changes with incidence of lifestyle advice and treatment for uncomplicated mild hypertension in primary care: a longitudinal cohort study in the Clinical Practice Research Datalink
Abstract
Objectives: Evidence to support initiation of pharmacological treatment in patients with uncomplicated (low risk) mild hypertension is inconclusive. As such, clinical guidelines are contradictory and healthcare policy has changed regularly. The aim of this study was to determine the incidence of lifestyle advice and drug therapy in this population and whether secular trends were associated with policy changes.
Design: Longitudinal cohort study.
Setting: Primary care practices contributing to the Clinical Practice Research Datalink in England.
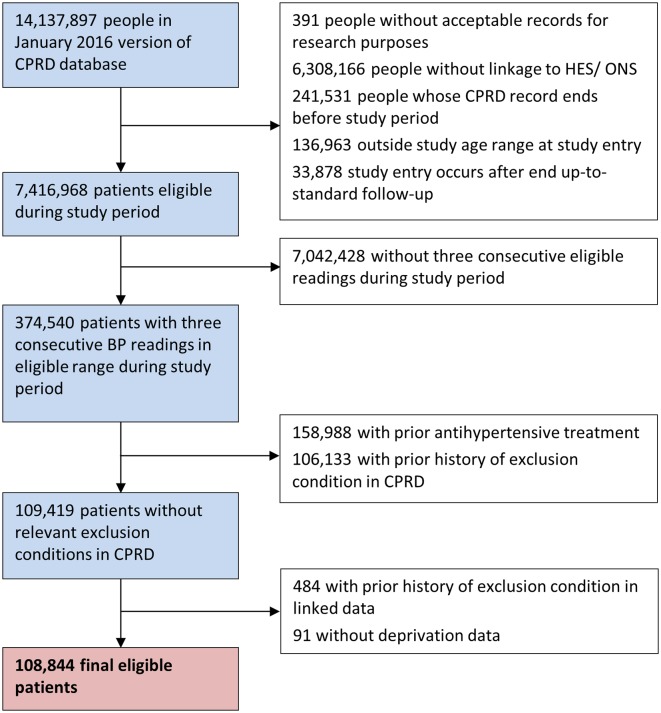
Participants: Data were extracted from the linked electronic health records of patients aged 18-74 years, with stage 1 hypertension (blood pressure between 140/90 and 159/99 mm Hg), no cardiovascular disease (CVD) risk factors and no treatment, from 1998 to 2015. Patients exited if follow-up records became unavailable, they progressed to stage 2 hypertension, developed a CVD risk factor or received lifestyle advice/treatment.
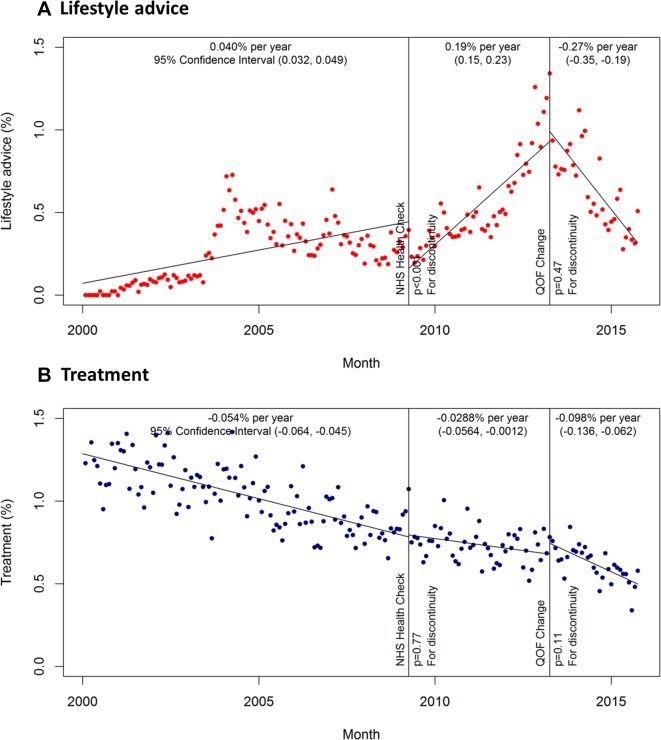
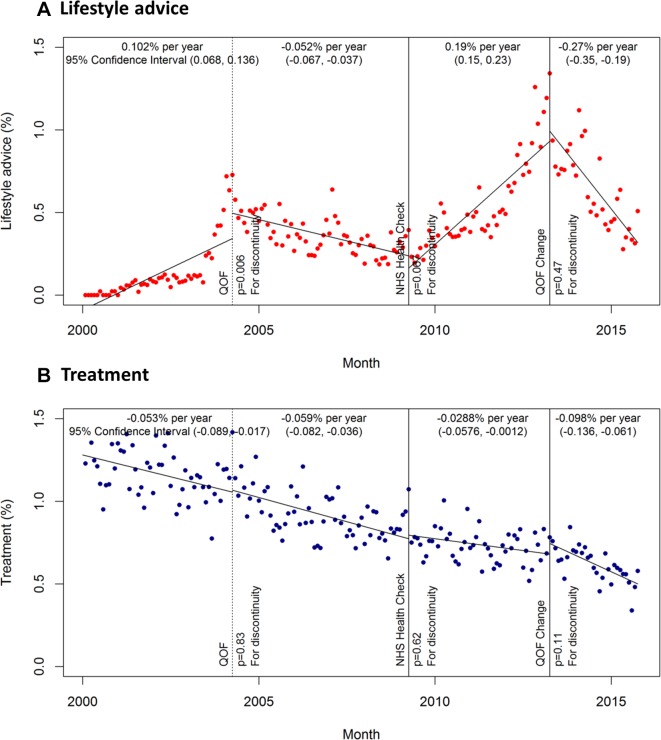
Primary outcome measures: The association between policy changes and incidence of lifestyle advice or treatment, examined using an interrupted time-series analysis.
Results: A total of 108 843 patients were defined as having uncomplicated mild hypertension (mean age 51.9±12.9 years, 60.0% female). Patientsspent a median 2.6 years (IQR 0.9-5.5) in the study, after which 12.2% (95% CI 12.0% to 12.4%) were given lifestyle advice, 29.9% (95% CI 29.7% to 30.2%) were prescribed medication and 19.4% (95% CI 19.2% to 19.6%) were given both. The introduction of the quality outcomes framework (QOF) and subsequent changes to QOF indicators were followed by significant increases in the incidence of lifestyle advice. Treatment prescriptions decreased slightly over time, but were not associated with policy changes.
Conclusions: Despite secular trends that accord with UK guidance, many patients are still prescribed treatment for mild hypertension. Adequately powered studies are needed to determine if this is appropriate.
Keywords: blood pressure; cardiovascular disease prevention; electronic health records; general practice; interrupted time series.
© Author(s) (or their employer(s)) 2018. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: RJS is a member of the CPRD’s Independent Scientific Advisory Committee (ISAC), but was not involved in the approval of this study.
Figures
References
-
- Lewington S, Clarke R, Qizilbash N, et al. . Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002;360:1903–13. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials