

Electronic healthcare databases in Europe: descriptive analysis of characteristics and potential for use in medicines regulation
- PMID: 30185579
- PMCID: PMC6129090
- DOI: 10.1136/bmjopen-2018-023090
Electronic healthcare databases in Europe: descriptive analysis of characteristics and potential for use in medicines regulation
Erratum in
-
Correction: Electronic healthcare databases in Europe: descriptive analysis of characteristics and potential for use in medicines regulation.BMJ Open. 2019 Feb 22;8(11):e023090corr1. doi: 10.1136/bmjopen-2018-023090corr1. BMJ Open. 2019. PMID: 30798300 Free PMC article. No abstract available.
Abstract
Objective: Electronic healthcare databases (EHDs) are useful tools for drug development and safety evaluation but their heterogeneity of structure, validity and access across Europe complicates the conduct of multidatabase studies. In this paper, we provide insight into available EHDs to support regulatory decisions on medicines.
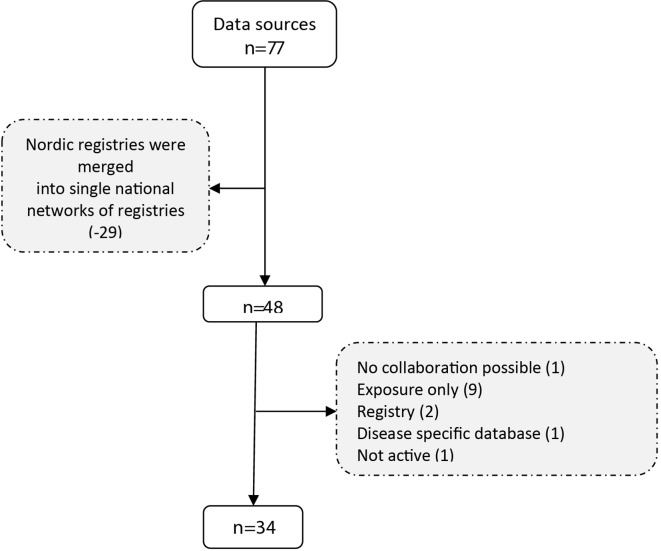
Methods: EHDs were identified from publicly available information from the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance resources database, textbooks and web-based searches. Databases were selected using criteria related to accessibility, longitudinal dimension, recording of exposure and outcomes, and generalisability. Extracted information was verified with the database owners.
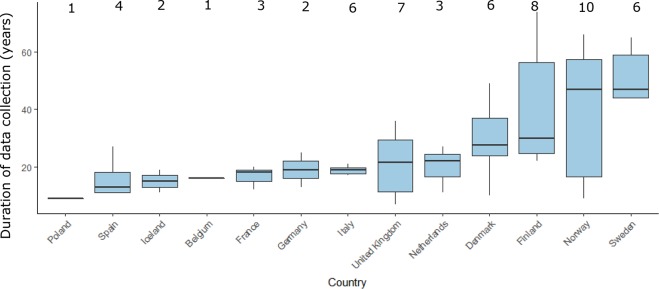
Results: A total of 34 EHDs were selected after applying key criteria relevant for regulatory purposes. The most represented regions were Northern, Central and Western Europe. The most frequent types of data source were electronic medical records (44.1%) and record linkage systems (29.4%). The median number of patients registered in the 34 data sources was 5 million (range 0.07-15 million) while the median time covered by a database was 18.5 years. Paediatric patients were included in 32 databases (94%). Completeness of information on drug exposure was variable. Published validation studies were found for only 17 databases (50%). Some level of access exists for 25 databases (73.5%), and 23 databases (67.6%) can be linked through a personal identification number to other databases with parent-child linkage possible in 7 (21%) databases. Eight databases (23.5%) were already transformed or were in the process of being transformed into a common data model that could facilitate multidatabase studies.
Conclusion: A Few European databases meet minimal regulatory requirements and are readily available to be used in a regulatory context. Accessibility and validity information of the included information needs to be improved. This study confirmed the fragmentation, heterogeneity and lack of transparency existing in many European EHDs.
Keywords: benefit-risk evaluation; electronic healthcare databases; post-authorisation studies; real-world data; regulatory science.
© Author(s) (or their employer(s)) 2018. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- Good pharmacovigilance practice. Module VIII. Post-authorisation safety studies. 2016. http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guidelin... (accessed 17 Nov 2017).
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources