

High-flow nasal cannula oxygen therapy alone or with non-invasive ventilation during the weaning period after extubation in ICU: the prospective randomised controlled HIGH-WEAN protocol
- PMID: 30185583
- PMCID: PMC6129104
- DOI: 10.1136/bmjopen-2018-023772
High-flow nasal cannula oxygen therapy alone or with non-invasive ventilation during the weaning period after extubation in ICU: the prospective randomised controlled HIGH-WEAN protocol
Abstract
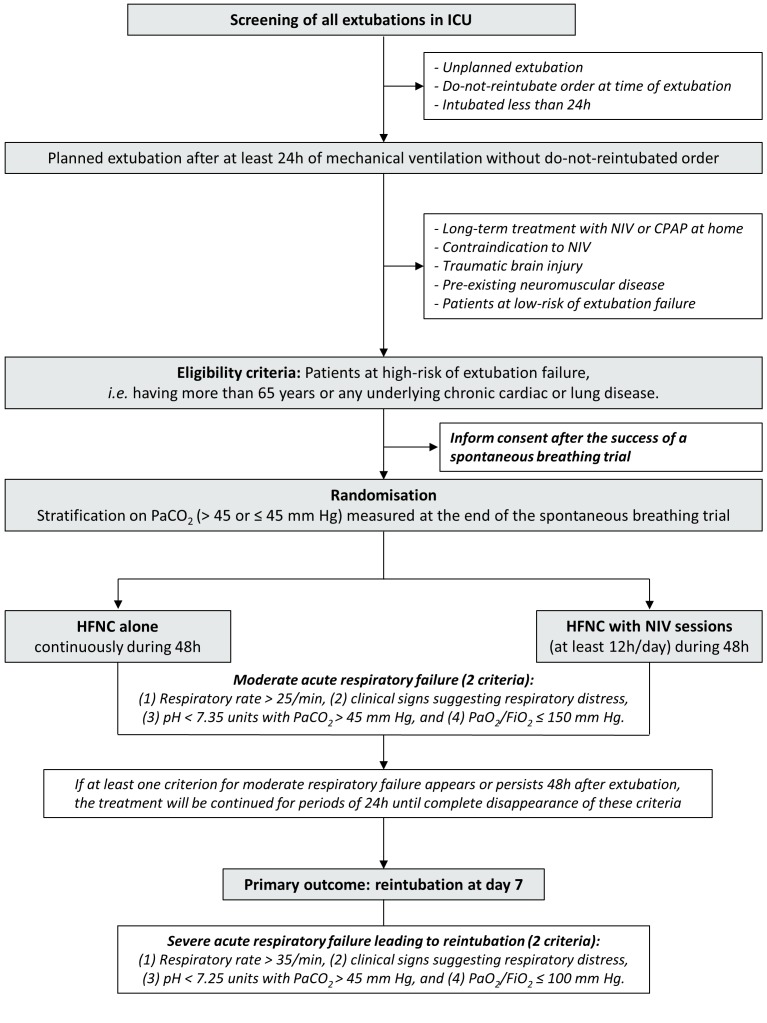
Introduction: Recent practice guidelines suggest applying non-invasive ventilation (NIV) to prevent postextubation respiratory failure in patients at high risk of extubation failure in intensive care unit (ICU). However, such prophylactic NIV has been only a conditional recommendation given the low certainty of evidence. Likewise, high-flow nasal cannula (HFNC) oxygen therapy has been shown to reduce reintubation rates as compared with standard oxygen and to be as efficient as NIV in patients at high risk. Whereas HFNC may be considered as an optimal therapy during the postextubation period, HFNC associated with NIV could be an additional means of preventing postextubation respiratory failure. We are hypothesising that treatment associating NIV with HFNC between NIV sessions may be more effective than HFNC alone and may reduce the reintubation rate in patients at high risk.
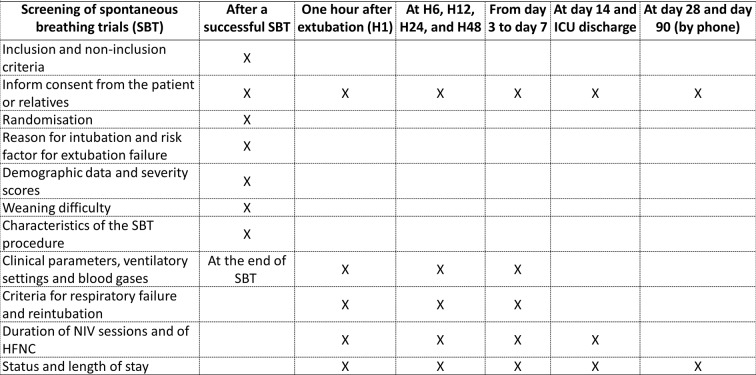
Methods and analysis: This study is an investigator-initiated, multicentre randomised controlled trial comparing HFNC alone or with NIV sessions during the postextubation period in patients at high risk of extubation failure in the ICU. Six hundred patients will be randomised with a 1:1 ratio in two groups according to the strategy of oxygenation after extubation. The primary outcome is the reintubation rate within the 7 days following planned extubation. Secondary outcomes include the number of patients who meet the criteria for moderate/severe respiratory failure, ICU length of stay and mortality up to day 90.
Ethics and dissemination: The study has been approved by the ethics committee and patients will be included after informed consent. The results will be submitted for publication in peer-reviewed journals.
Trial registration number: NCT03121482.
Keywords: adult intensiv & critical care; clinical trials.
© Author(s) (or their employer(s)) 2018. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: AWT and J-DR report travel expenses coverage to attend scientific meetings by Fisher & Paykel. AD and SE received research grants from Fisher & Paykel. J-PF reports consulting fees from Fisher & Paykel.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical