

Improved outcomes in PI3K-pathway-altered metastatic HPV oropharyngeal cancer
- PMID: 30185662
- PMCID: PMC6171803
- DOI: 10.1172/jci.insight.122799
Improved outcomes in PI3K-pathway-altered metastatic HPV oropharyngeal cancer
Abstract
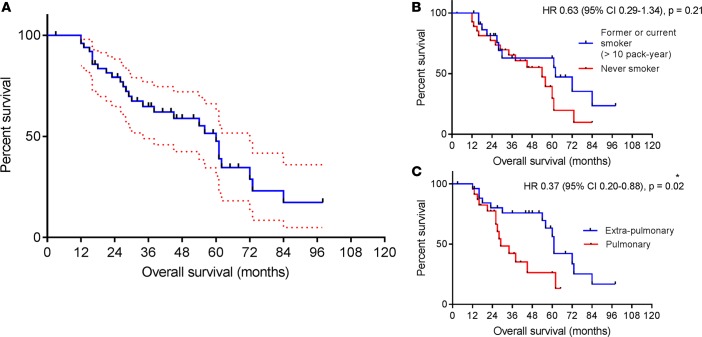
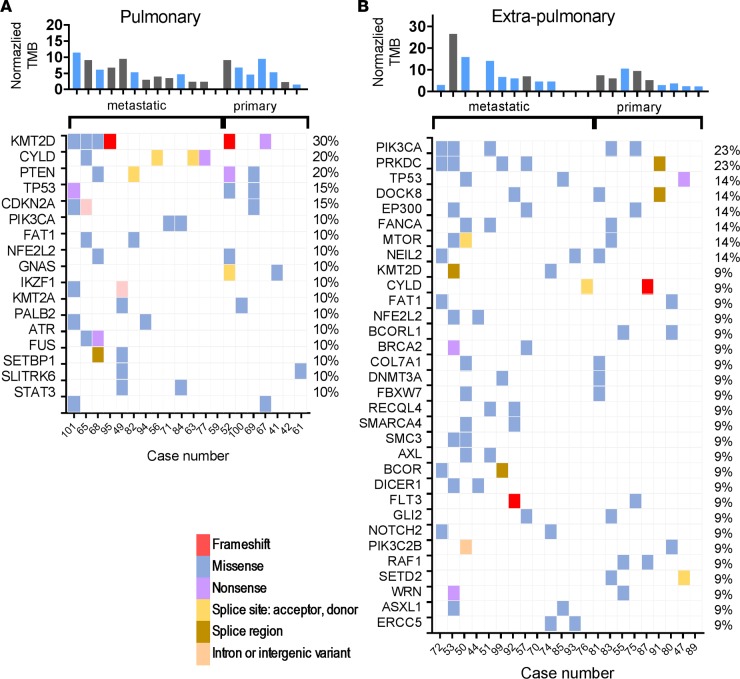
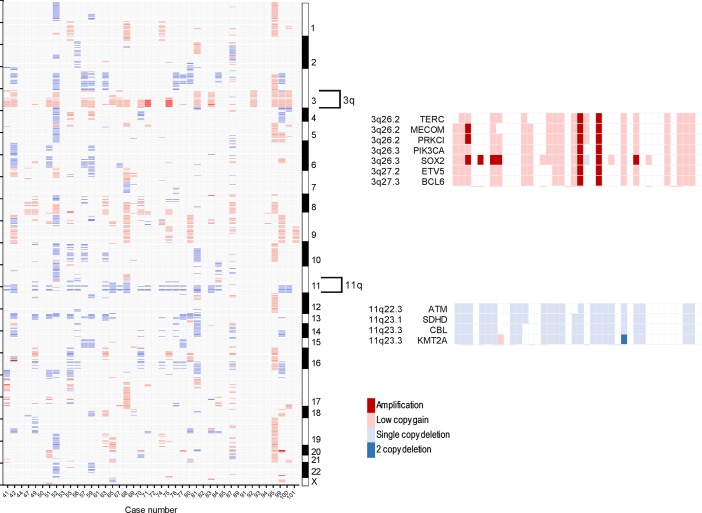
While it has been recognized that human papillomavirus-associated (HPV-associated) oropharyngeal cancer (OPC) portends an improved prognosis, distinct patterns of disease recurrence have emerged. Molecular characterization of this subset of HPV patients remains unexplored. We evaluated 52 metastatic HPV+ OPC patients from our institution and paired massively parallel sequencing data with clinical parameters and survival outcomes in 81% of patients. Genomic data were then compared with 2 molecularly defined, curable HPV+ cohorts. Metastatic HPV+ OPC patients with pulmonary-only metastases demonstrated worse outcomes. Nonexclusive somatic alterations in KMT2D and PIK3CA were most frequent, with PRKDC alterations occurring at higher frequency when compared with all sequenced HPV+ OPC patients. PI3K pathway alterations were associated with improved outcomes among metastatic HPV+ OPC patients. We demonstrate subtle differences in the mutational landscape between curable and metastatic HPV+ OPC populations, with a trend towards more frequent DNA repair protein alterations in the latter. We demonstrate improved outcomes when PI3K pathway alterations are present in these patients. We provide molecular insights for this important HPV+ subgroup that have significant therapeutic implications.
Keywords: Genetics; Head & neck cancer; Molecular genetics; Oncology.
Conflict of interest statement
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
