

Ultrasound-guided continuous fascia iliaca compartment block for pre-operative pain control in very elderly patients with hip fracture: A randomized controlled trial
- PMID: 30186422
- PMCID: PMC6122427
- DOI: 10.3892/etm.2018.6417
Ultrasound-guided continuous fascia iliaca compartment block for pre-operative pain control in very elderly patients with hip fracture: A randomized controlled trial
Abstract
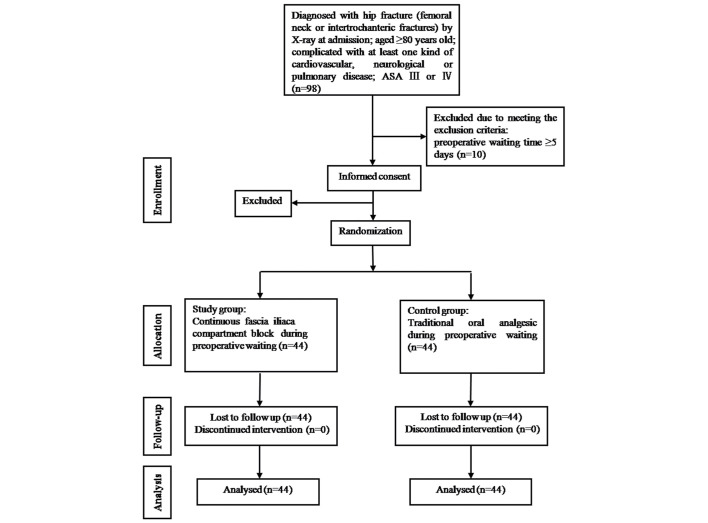
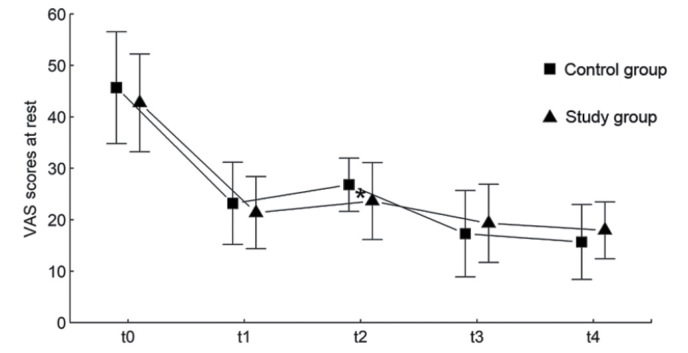
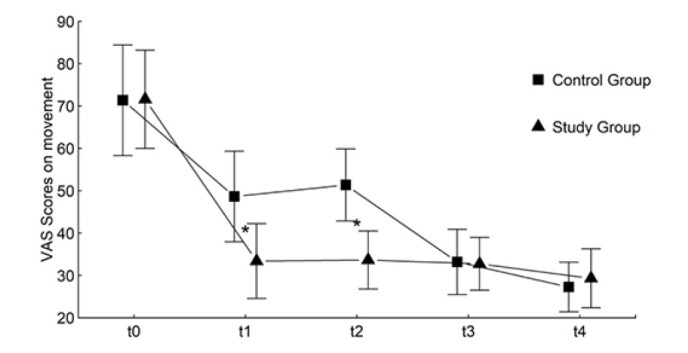
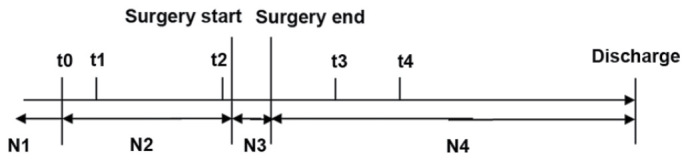
The present study presented the results of a prospective, randomized controlled trial. The present study enrolled 98 very elderly patients with hip fractures, complicated with at least one cardiovascular, neurological or pulmonary disease, of whom 10 patients were excluded. A total of 88 patients were randomly assigned into 2 groups: i) The control group, receiving traditional analgesia including 50 mg Tramadol and 500 mg paracetamol orally three times a day from admission to surgery; and ii) the study group, receiving ultrasound-guided continuous fascia iliaca compartment block (CFICB), a single 50 ml 0.4% ropivacaine injection with continuous infusion of 0.2% ropivacaine at a dose of 5 ml/h from admission to surgery. The primary outcome measure of pain relief or pain intensity was assessed preoperatively and up to 48 h postoperatively using a visual analog scale (VAS). The results of the present study indicated that in the preoperative period, in the morning of the day of surgery, the VAS pain at rest scores were lower in the study group compared with the control group (P=0.023). The VAS passive movement scores of the study group were also significantly lower compared with the control group 1 h following analgesia at the time of admission (P<0.05) and in the morning of the day of surgery (P<0.05). Scores for patients' satisfaction with the analgesic regimen in the preoperative period were greater in the study group compared with the control group (P<0.001). There was no difference in analgesia-associated side effects between groups. Duration of hospital stay of patients in the control group was significantly longer compared with the study group (P=0.001). Patients in the study group were less likely to have increased complications compared with patients in the control group over the N2-N4 period (from preoperative period to after surgery; P=0.016). The present study concluded that ultrasound guided CFICB was an effective method of providing analgesia for very elderly (≥80 years old) with hip fracture.
Keywords: analgesia; geriatrics; hip fracture; pain; ultrasound-guided fascia iliaca compartment block.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources