

Reversible splenial lesion syndrome associated with acute Mycoplasma pneumoniae-associated encephalitis: A report of four cases and literature review
- PMID: 30186453
- PMCID: PMC6122408
- DOI: 10.3892/etm.2018.6387
Reversible splenial lesion syndrome associated with acute Mycoplasma pneumoniae-associated encephalitis: A report of four cases and literature review
Abstract
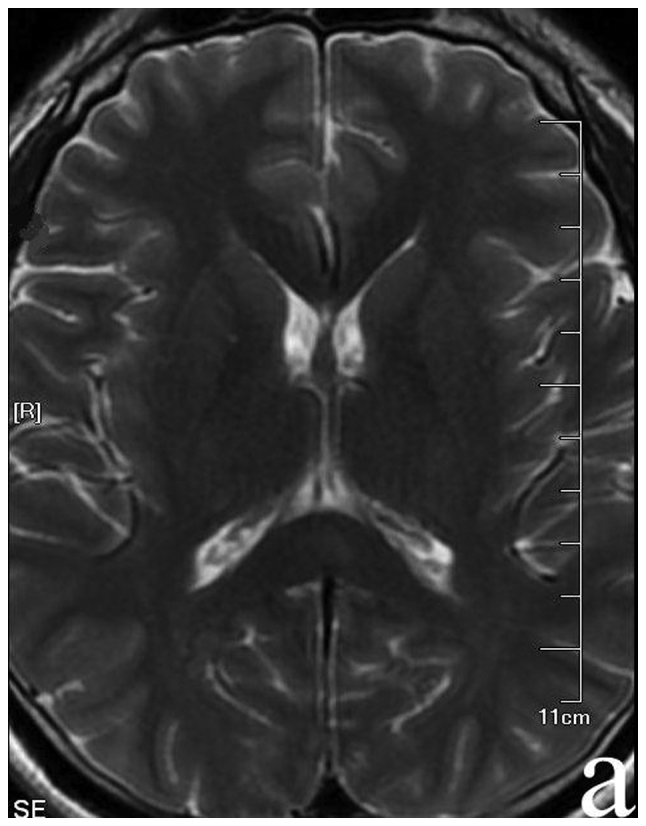
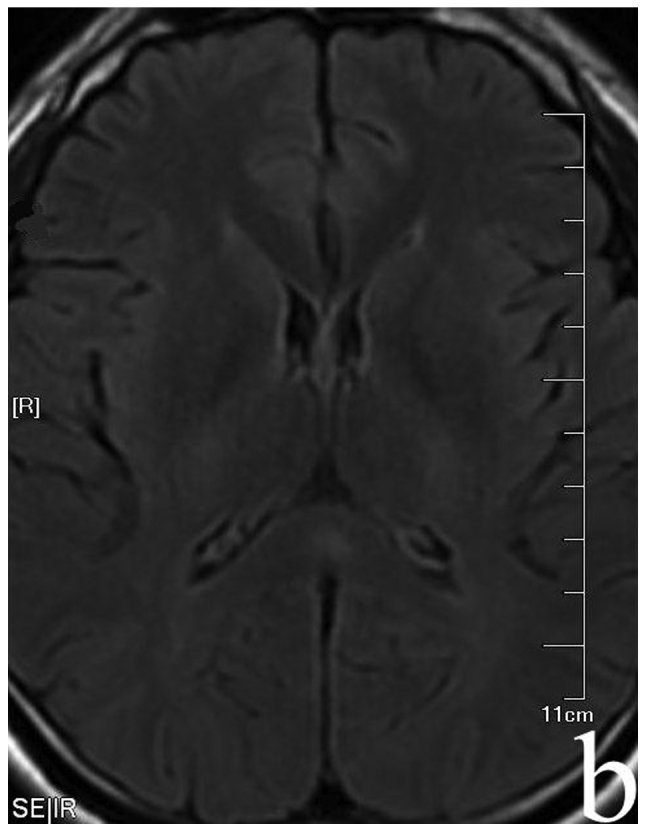
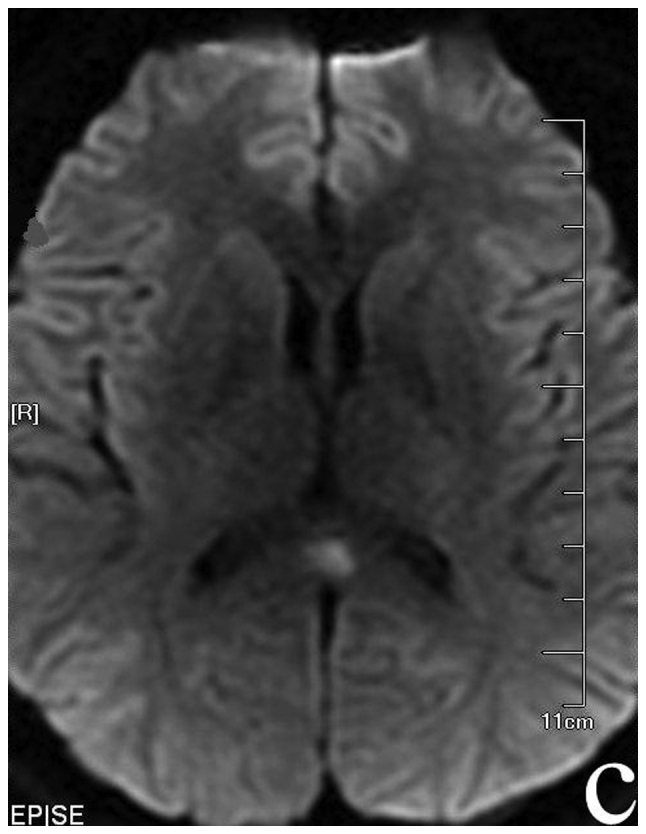
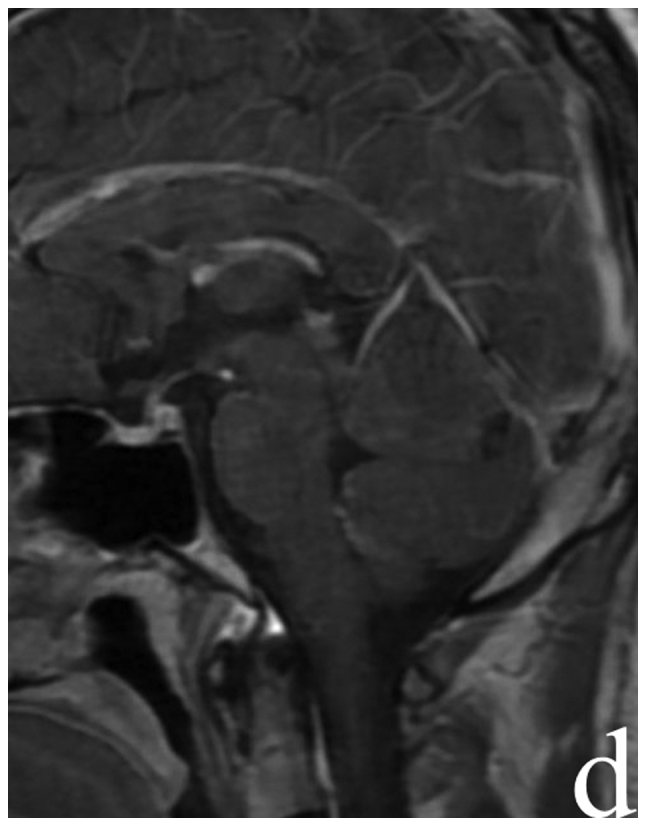
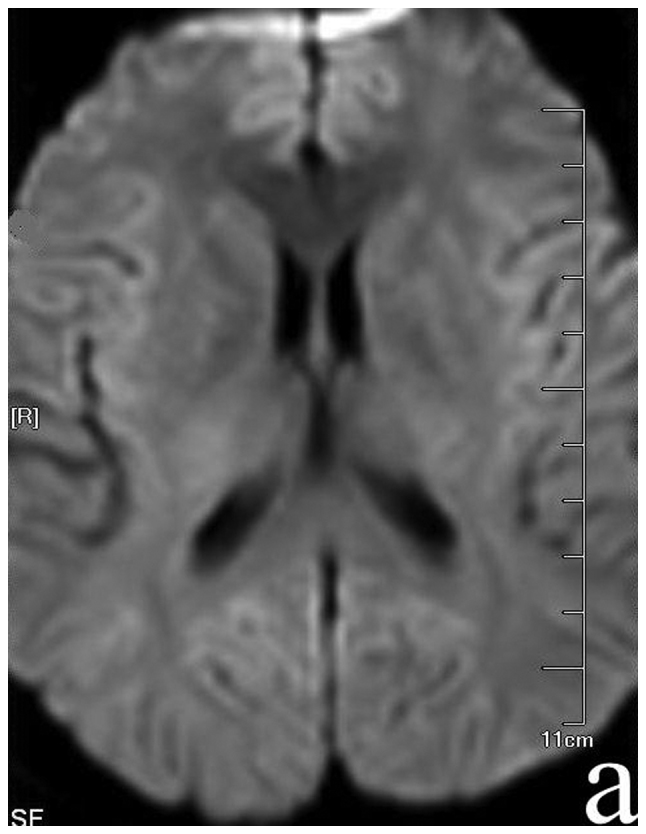
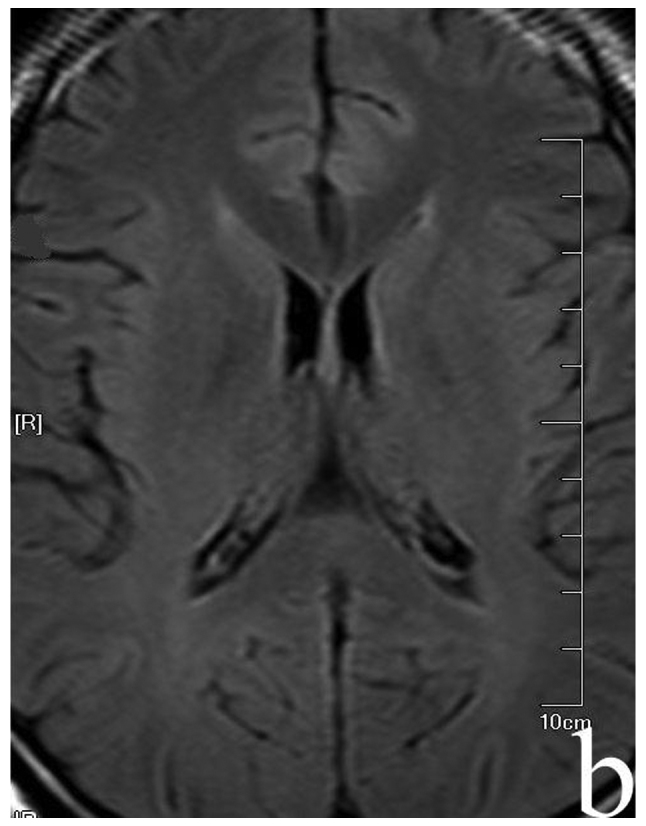
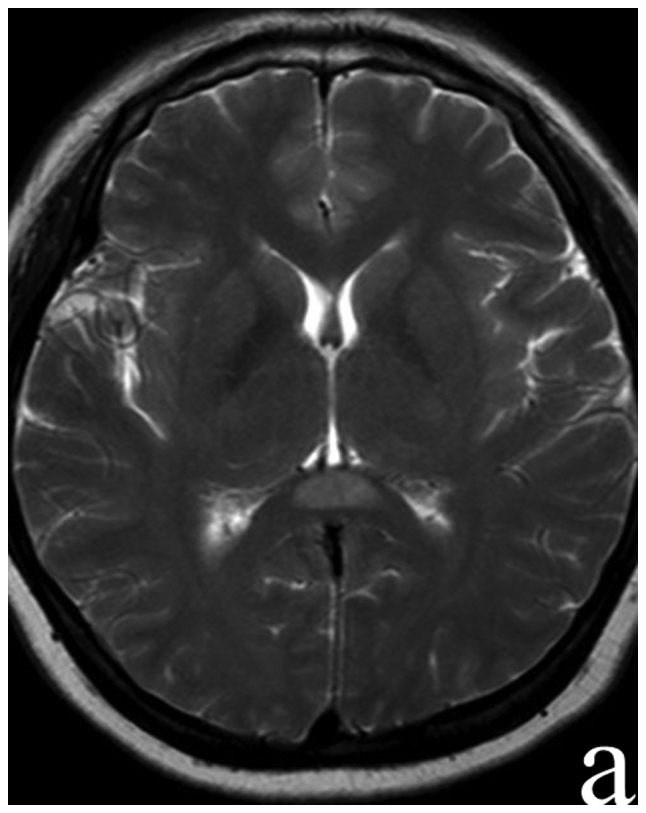
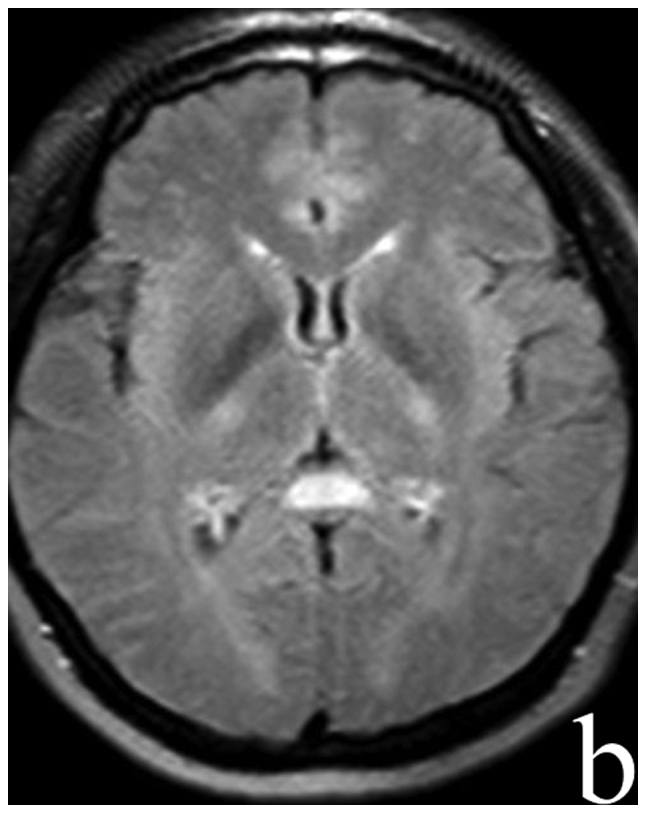
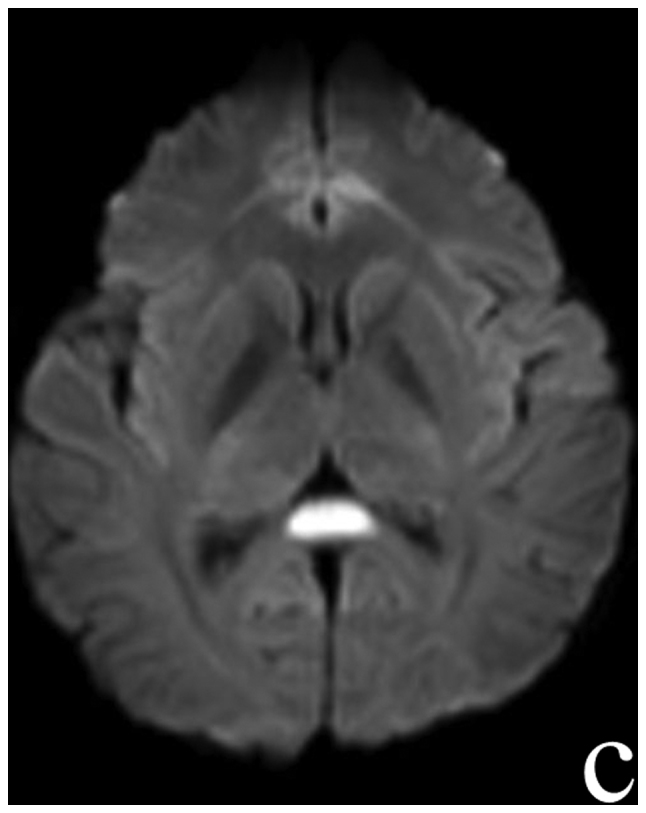
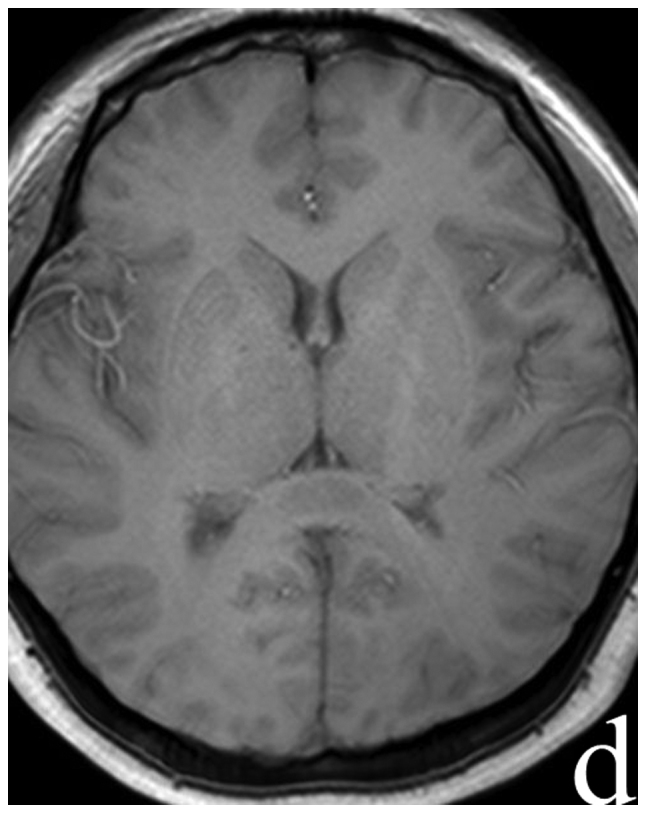
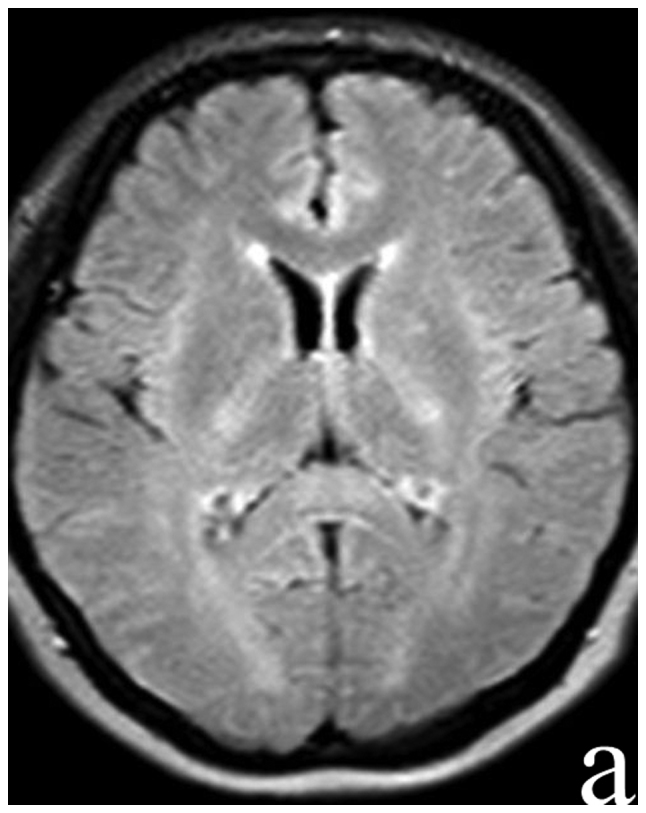
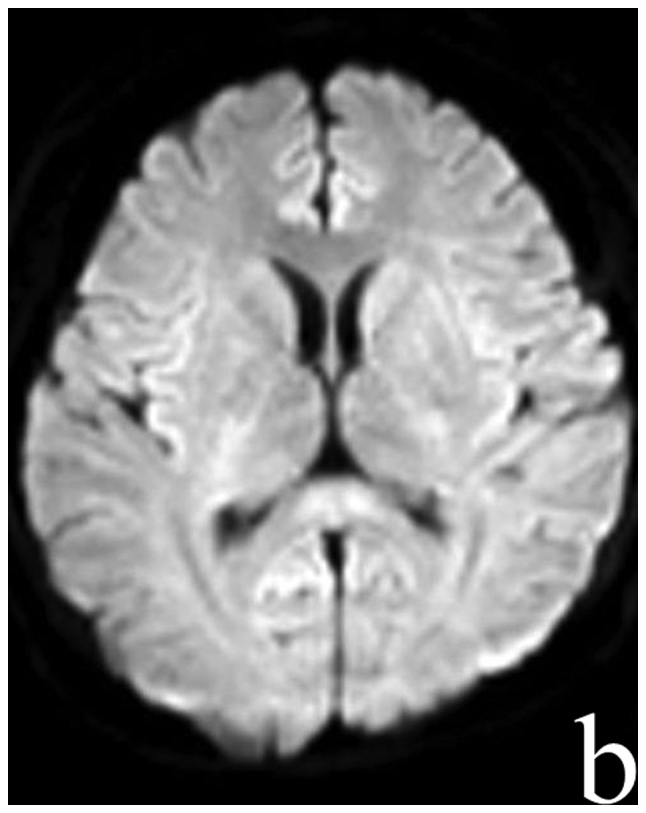
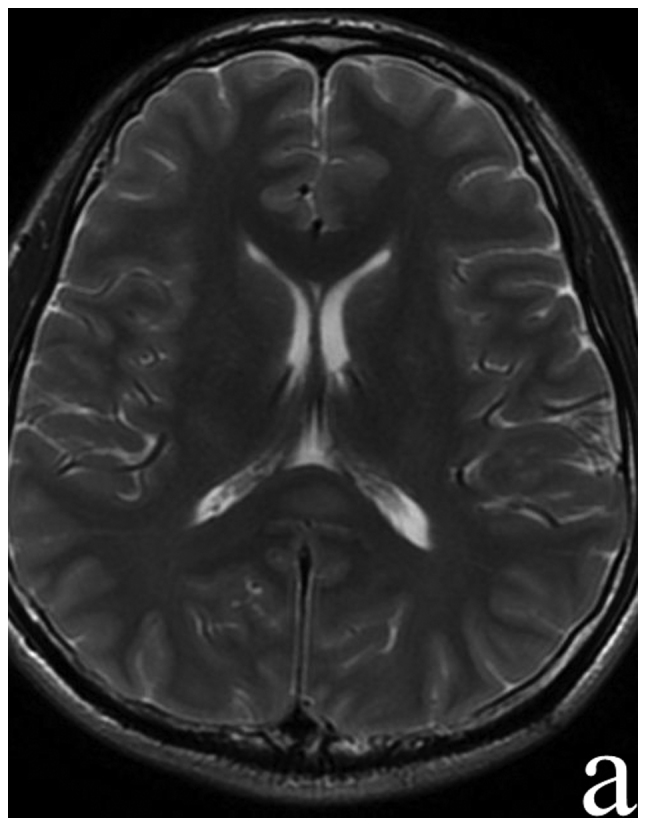
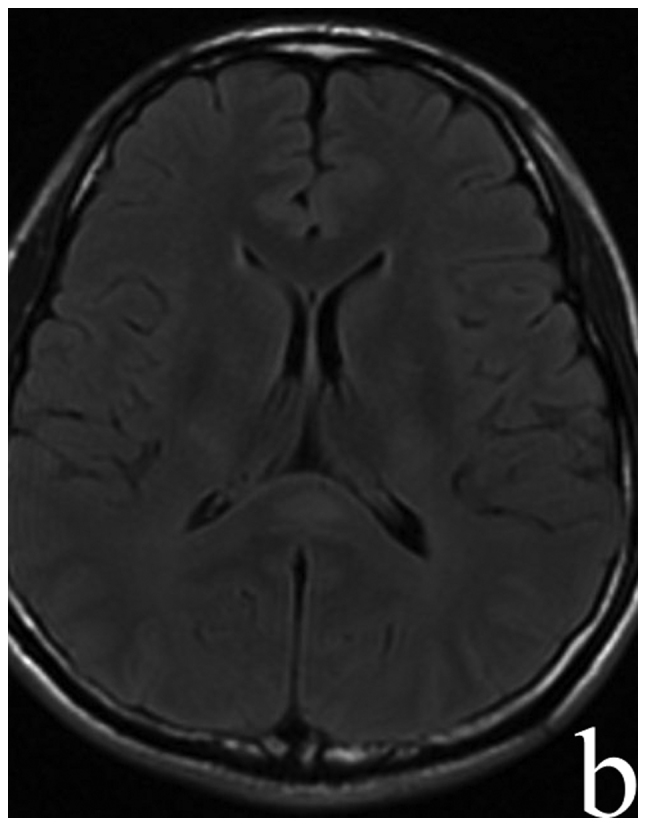
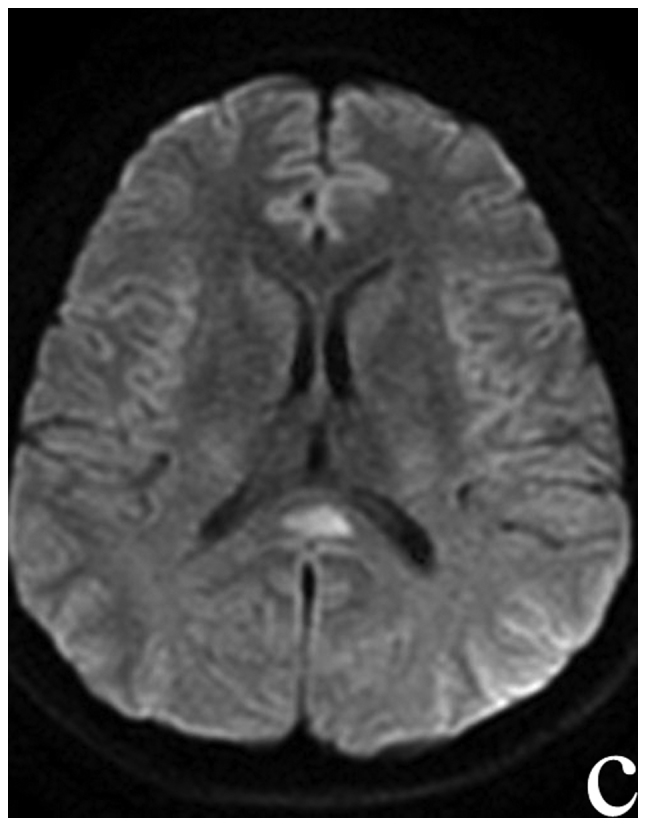
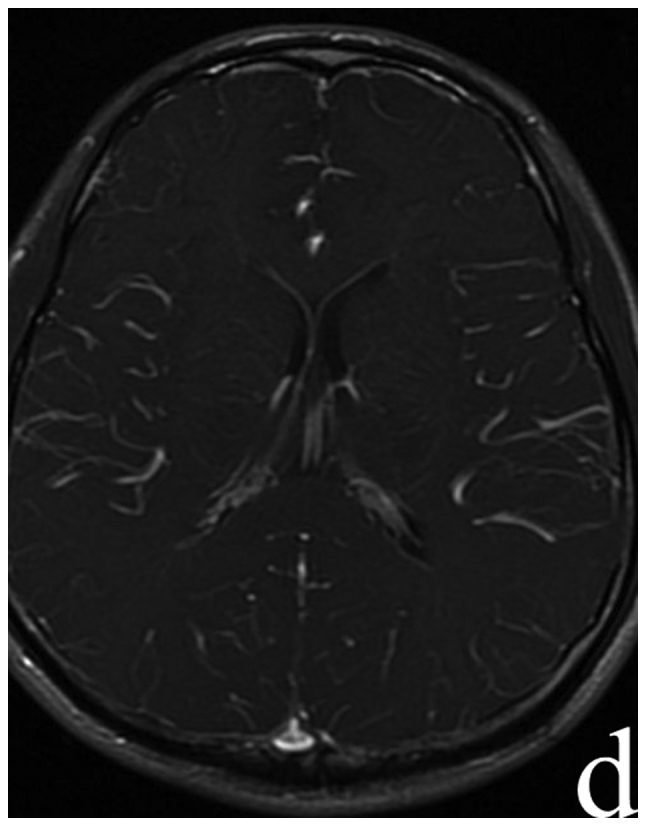
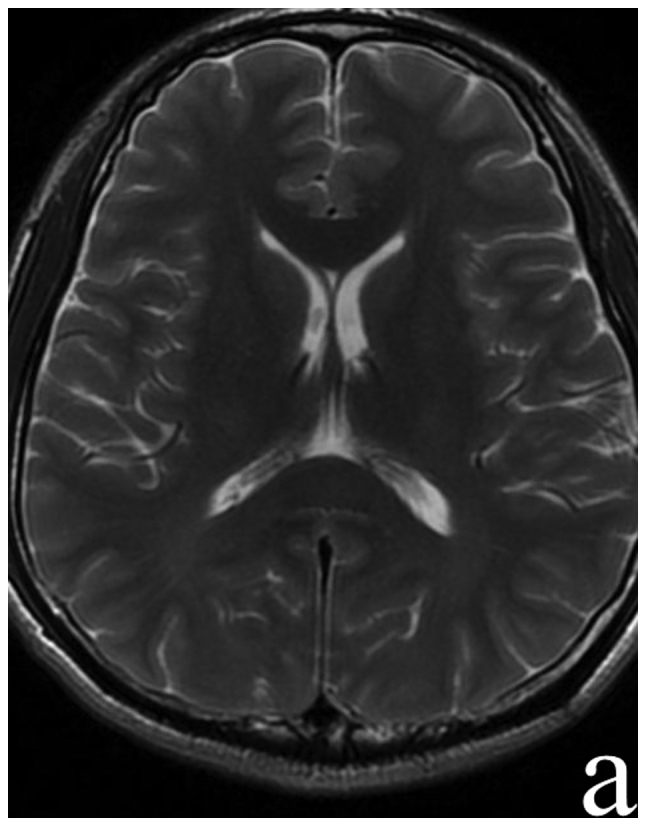
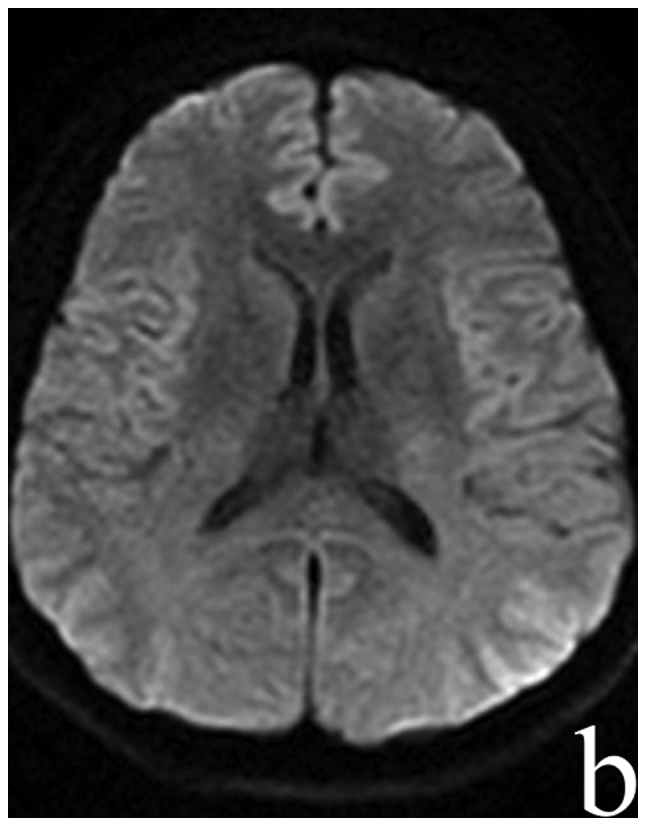
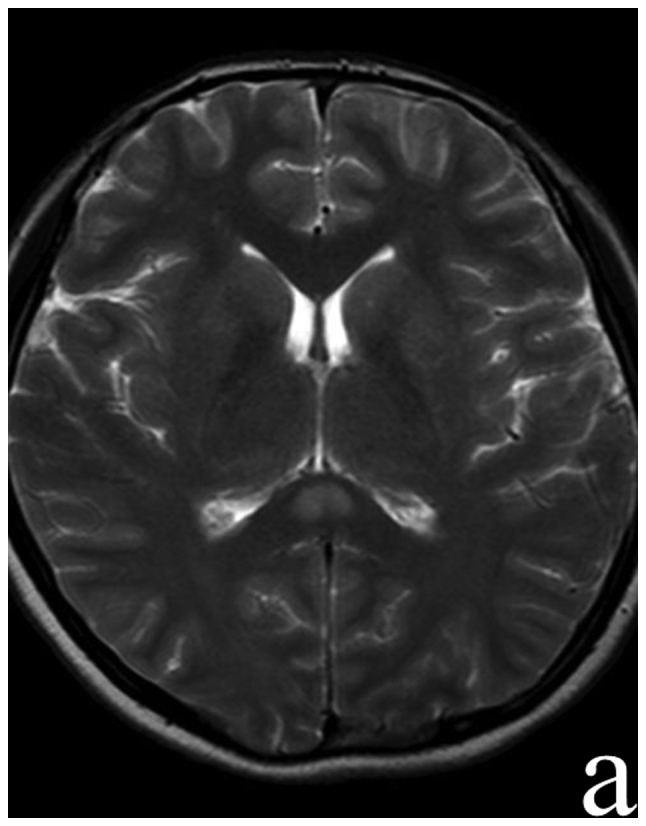
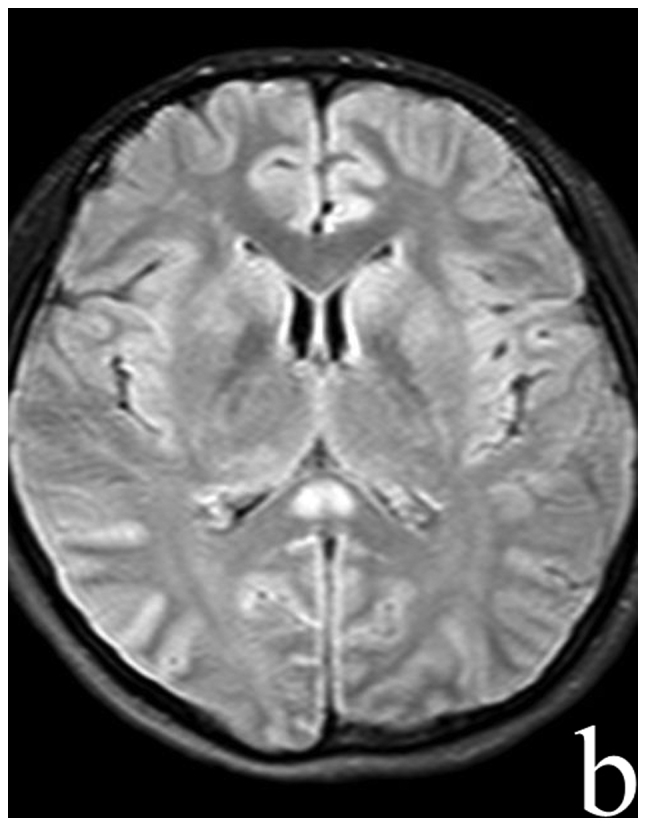
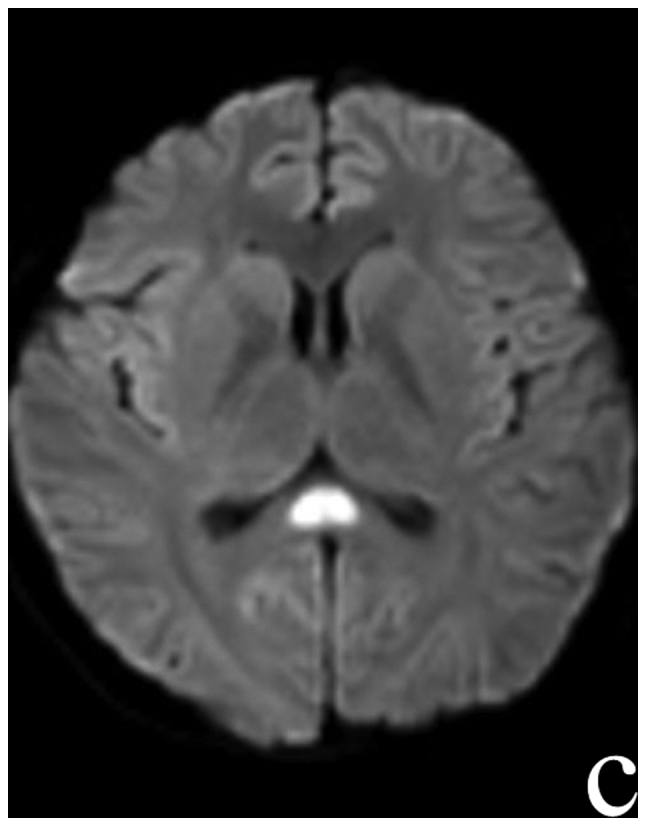
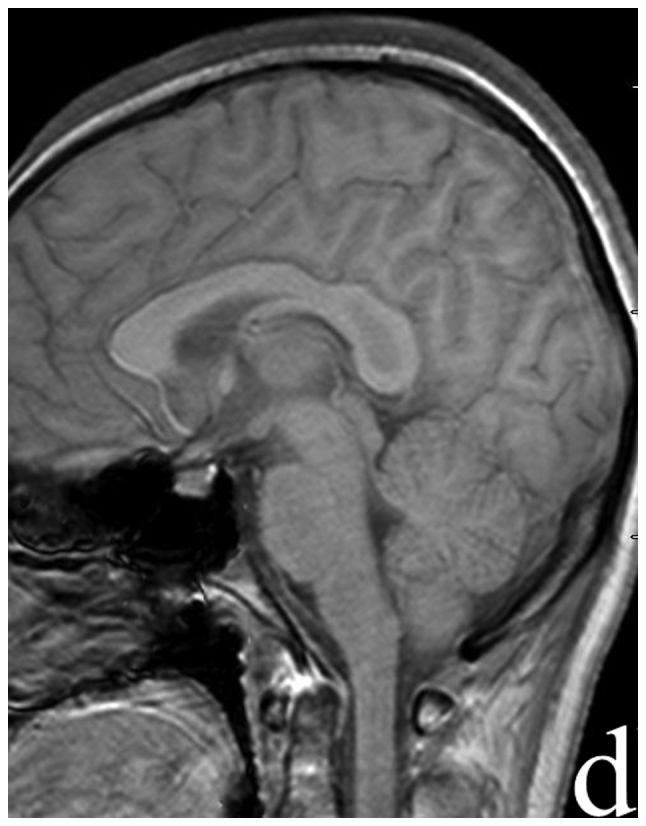
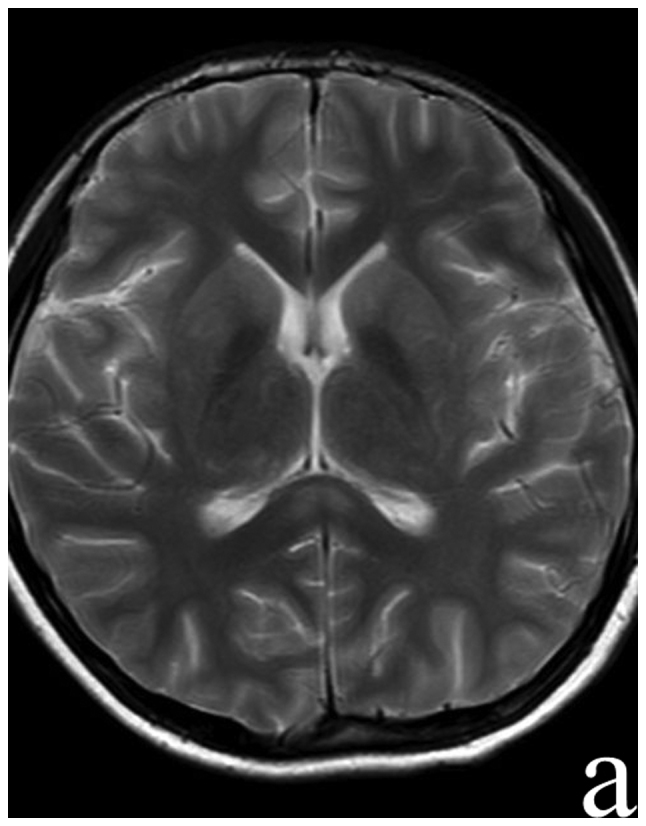
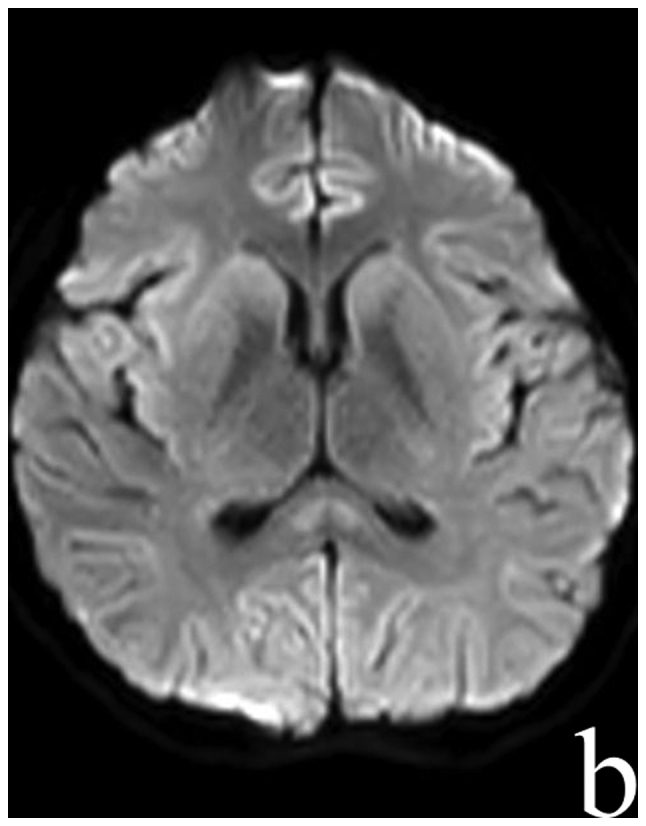
Reversible splenial lesion syndrome (RESLES) is a rare clinico-radiological syndrome that is defined as reversible lesions that involve the splenium of the corpus callosum (SCC). RESLES has been reported in patients with a broad spectrum of diseases and conditions, including infections, hypoglycemia and poisoning. The present report described four RESLES cases triggered by Mycoplasma pneumoniae (M. pneumoniae) and discussed the associated diagnostic challenges. Four cases of acute M. pneumoniae-associated encephalitis that displayed RESLES were reviewed. The clinical presentations were nonspecific in these patients. However, magnetic resonance imaging (MRI) revealed consistent lesions in the SCC with a hyperintensity in diffusion-weighted imaging (DWI) and hypointensities in T1WI, which disappeared after a variable lapse. Treatment with azithromycin or combined treatment with immunomodulatory agents if necessary led to a good prognosis. The present findings indicated that radiological diagnosis of RESLES should be considered in patients with M. pneumoniae-associated encephalitis. Furthermore, serum Mycoplasma antibody is important for the diagnosis of M. pneumoniae-associated encephalitis.
Keywords: Mycoplasma pneumoniae-associated encephalitis; magnetic resonance imaging; reversible splenial lesion syndrome; serum antibody.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials