

A case of excessive femoral anteversion which caused instability of the medial collateral ligament of the knee joint
- PMID: 30186601
- PMCID: PMC6123062
- DOI: 10.1016/j.amsu.2018.08.018
A case of excessive femoral anteversion which caused instability of the medial collateral ligament of the knee joint
Abstract
Introduction: The most cases of excessive femoral anteversion may be asymptomatic, because the he hip joint is a ball joint. However, when the hip, knee, or ankle joint is in a pathological state, excessive femoral anteversion may not be compensated for and induce symptoms.
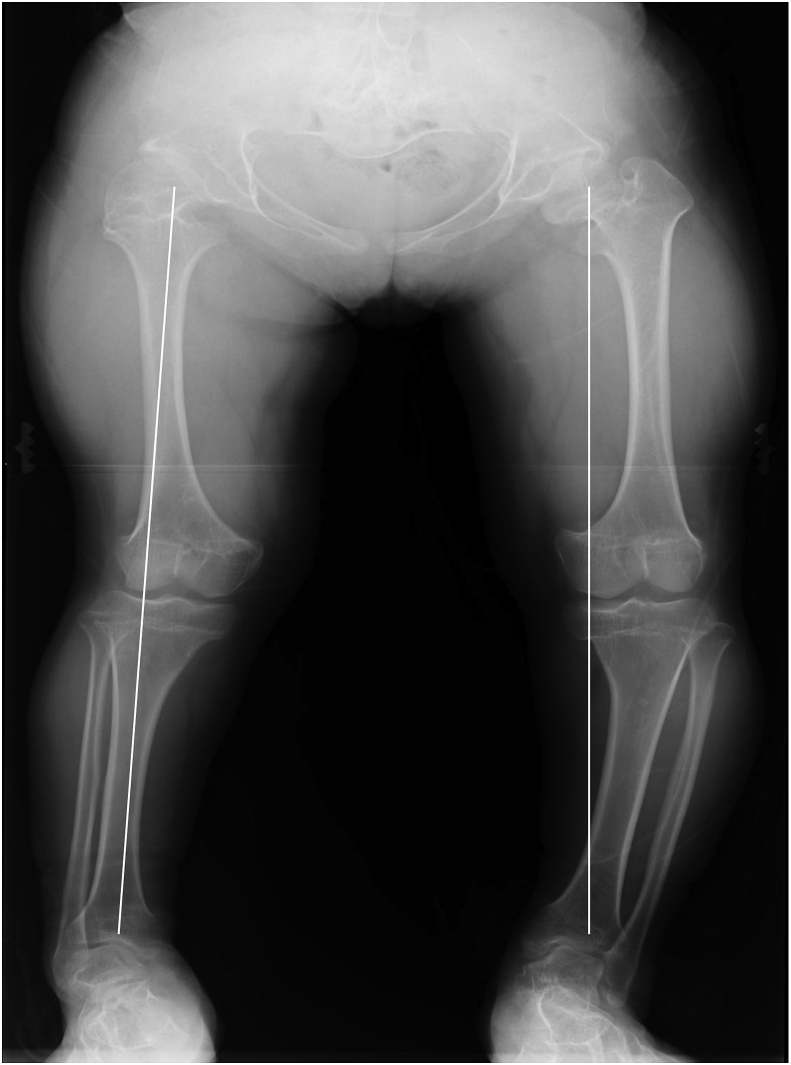
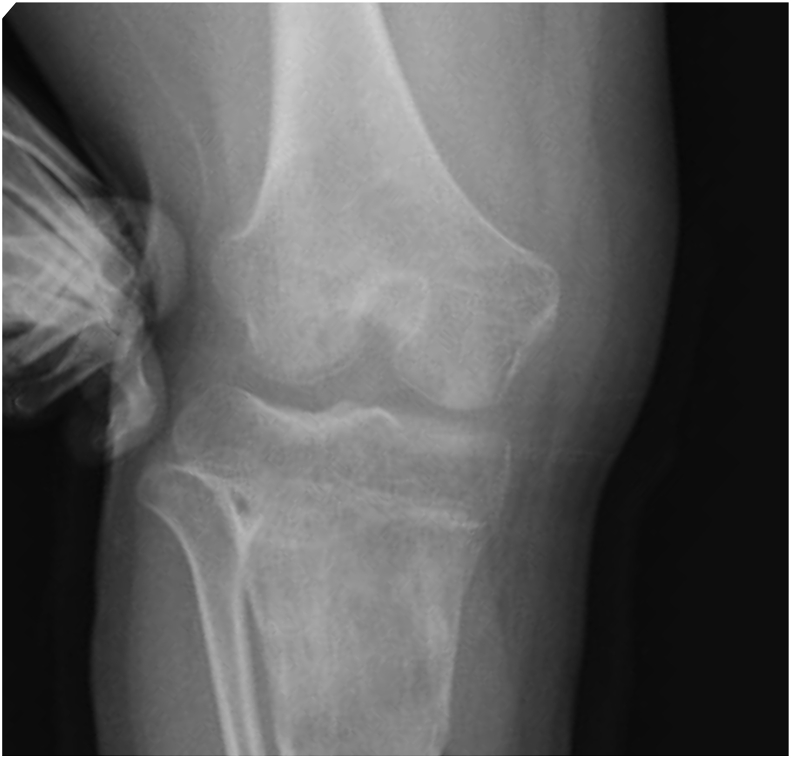
Case report: A 16-year-old female with achondroplasia. Medullary compression by the odontoid process caused right hemiplegia at 10 months after birth and equinus foot concomitantly developed. At 14 years old, right knee pain developed during walking. For treatment, firstly, tenodesis of medial collateral ligament of the knee joint (MCL) was performed. Oblique osteotomy was applied to the proximal MCL attachment site over the distal tibial tuberosity, followed by simple limb lengthening, which improved knee instability. To prevent recurrence of knee instability, varus and derotationosteotomy of the femur and Vulpius procedure (triceps surae muscle lengthening) were additionally performed, and gait stabilized after surgery.
Discussion: Regarding the pathogenesis, her gait was originally in-toeing because of excessive femoral anteversion, but the lower leg did not internally rotate during walking because of equinus foot, and the foot grounded in an externally rotated position, loading burdens on the MCL. This condition may have gradually caused instability of the knee over the years.
Conclusion: We surgically treated the patient with knee joint valgus instability caused by excessive femoral anteversion and equinus foot and achieved a favorable outcome.
Keywords: Derotation osteotomy of femur; Equinus foot; Excessive femoral anteversion; Laxity of medial collateral ligament; Limb lengthening; case report.
Figures









Similar articles
-
Femoral Component External Rotation Affects Knee Biomechanics: A Computational Model of Posterior-stabilized TKA.Clin Orthop Relat Res. 2018 Jan;476(1):113-123. doi: 10.1007/s11999.0000000000000020. Clin Orthop Relat Res. 2018. PMID: 29529625 Free PMC article.
-
Increased femoral anteversion is associated with inferior clinical outcomes after MPFL reconstruction and combined tibial tubercle osteotomy for the treatment of recurrent patellar instability.Knee Surg Sports Traumatol Arthrosc. 2020 Jul;28(7):2261-2269. doi: 10.1007/s00167-019-05818-3. Epub 2019 Dec 4. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 31797022
-
Proximal femoral derotation osteotomy for idiopathic excessive femoral anteversion and intoeing gait.SICOT J. 2017;3:49. doi: 10.1051/sicotj/2017033. Epub 2017 Jul 4. SICOT J. 2017. PMID: 28675371 Free PMC article.
-
Management of medial collateral ligament laxity.Orthop Clin North Am. 1994 Jul;25(3):527-32. Orthop Clin North Am. 1994. PMID: 8028893 Review.
-
Role of surgery in the management of lesions of the medial collateral ligament of the ankle.Orthop Traumatol Surg Res. 2020 Dec;106(8S):S195-S199. doi: 10.1016/j.otsr.2020.08.005. Epub 2020 Sep 6. Orthop Traumatol Surg Res. 2020. PMID: 32900668 Review.
References
-
- Agha R.A., Fowler A.J., Saetta A., Barai I., Rajmohan S., Orgill D.P., for the SCARE Group The SCARE Statement: consensus-based surgical case report guidelines. Int. J. Surg. 2016;34:180–186. - PubMed
-
- Staheli L.T. Torsion—treatment indications. Clin Orthop Res. 1989;247:61–66. - PubMed
-
- Paley D., Bhatnagar J., Herzenberg J.E., Bhave A. New procedures for Tightening knee collateral ligaments in conjunction with knee realignment osteotomy. Orthop. Clin. N. Am. 1994;25:533–555. - PubMed
-
- Bruce W.D., Stevens P.M. Surgical correction of miserable malalignment syndrome. J. Pediatr. Orthop. 2004;24:392–396. - PubMed
-
- Paley D. Malalignment due to ligamentous laxity of the knee. In: Herzenberg J.E., Paley D., editors. Principles of Deformity Correction. Springer; New York: 2002. pp. 451–464.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
