

Imaging in Lyme neuroborreliosis
- PMID: 30187265
- PMCID: PMC6206375
- DOI: 10.1007/s13244-018-0646-x
Imaging in Lyme neuroborreliosis
Abstract
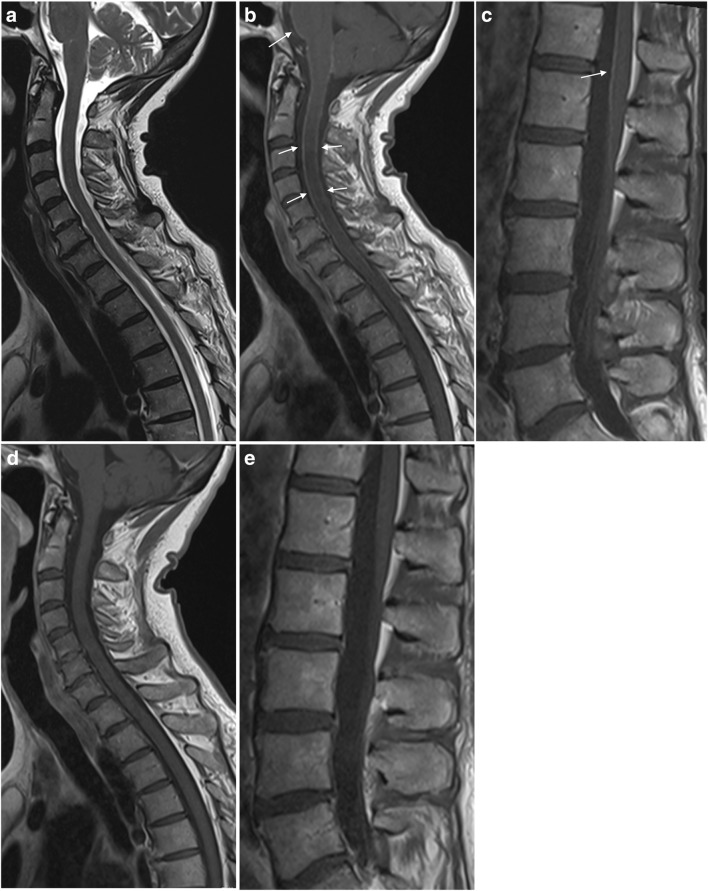
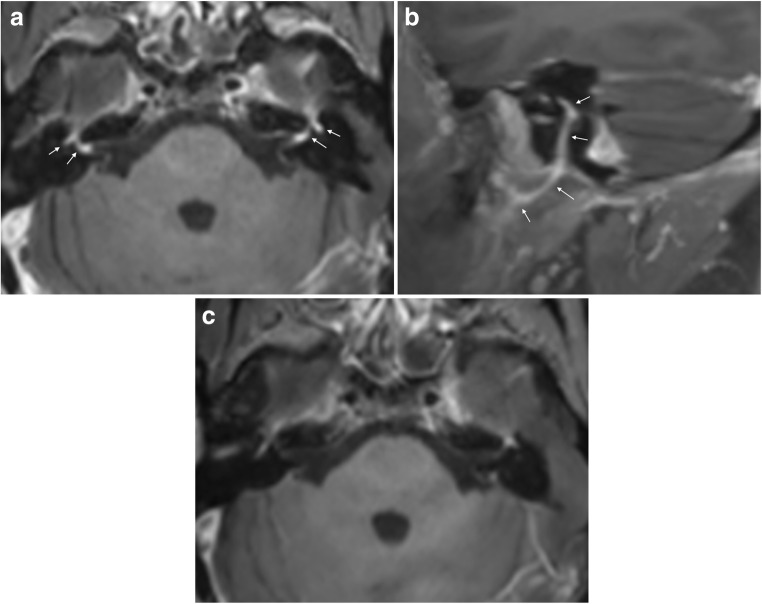
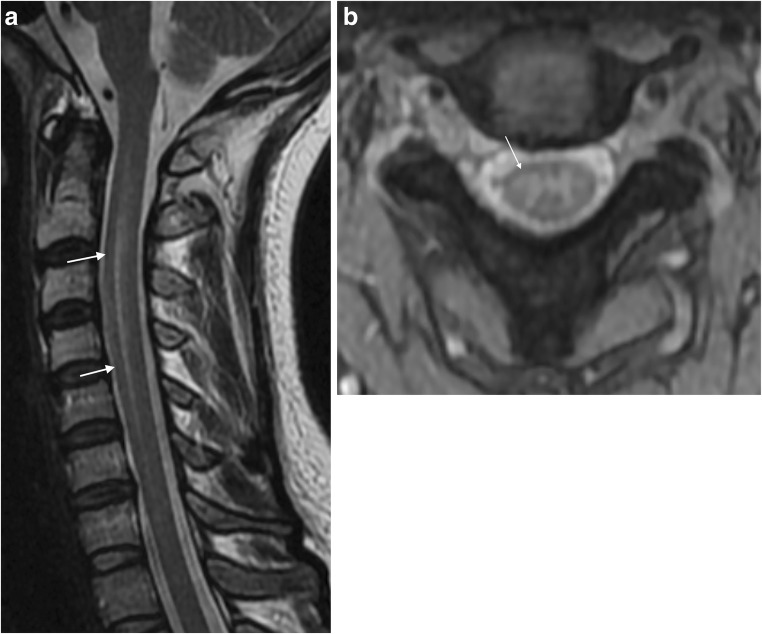
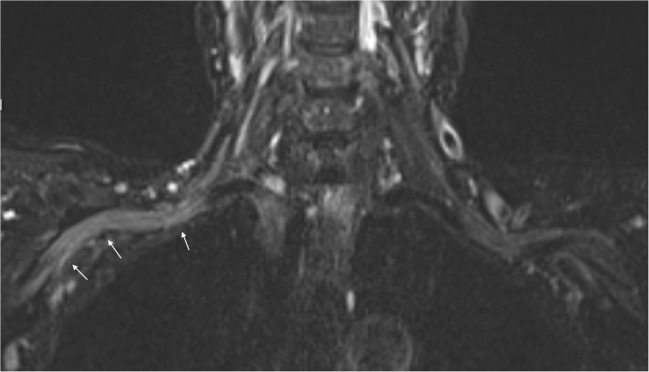
Lyme neuroborreliosis (LNB) is a tick-borne spirochetal infection with a broad spectrum of imaging pathology. For individuals who live in or have travelled to areas where ticks reside, LNB should be considered among differential diagnoses when clinical manifestations from the nervous system occur. Radiculitis, meningitis and facial palsy are commonly encountered, while peripheral neuropathy, myelitis, meningoencephalitis and cerebral vasculitis are rarer manifestations of LNB. Cerebrospinal fluid (CSF) analysis and serology are key investigations in patient workup. The primary role of imaging is to rule out other reasons for the neurological symptoms. It is therefore important to know the diversity of possible imaging findings from the infection itself. There may be no imaging abnormality, or findings suggestive of neuritis, meningitis, myelitis, encephalitis or vasculitis. White matter lesions are not a prominent feature of LNB. Insight into LNB clinical presentation, laboratory test methods and spectrum of imaging pathology will aid in the multidisciplinary interaction that often is imperative to achieve an efficient patient workup and arrive at a correct diagnosis. This article can educate those engaged in imaging of the nervous system and serve as a comprehensive tool in clinical cases. KEY POINTS: • Diagnostic criteria for LNB emphasise exclusion of an alternative cause to the clinical symptoms. • MRI makes a crucial contribution in the diagnosis and follow-up of LNB. • MRI may have normal findings, or show neuritis, meningitis, myelitis, encephalitis or vasculitis. • White matter lesions are not a prominent feature of LNB.
Keywords: Encephalitis; Lyme neuroborreliosis; MRI; Myelitis; Neuritis.
Conflict of interest statement
Mona K Beyer received minor grants or speaker’s fees from Biogen Idec, Merck and Novartis. Hanne F. Harbo received minor grants or speaker’s fees from Biogen, Sanofi Genzyme, Merck, Novartis and Teva. The other authors do not report any disclosures.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
