

High-flow nasal oxygen versus noninvasive ventilation in adult patients with cystic fibrosis: a randomized crossover physiological study
- PMID: 30187270
- PMCID: PMC6125258
- DOI: 10.1186/s13613-018-0432-4
High-flow nasal oxygen versus noninvasive ventilation in adult patients with cystic fibrosis: a randomized crossover physiological study
Abstract
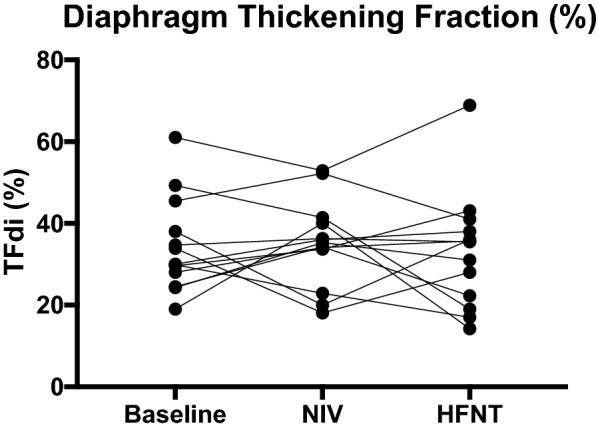
Background: Noninvasive ventilation (NIV) is the first-line treatment of adult patients with exacerbations of cystic fibrosis (CF). High-flow nasal oxygen therapy (HFNT) might benefit patients with hypoxemia and can reduce physiological dead space. We hypothesized that HFNT and NIV would similarly reduce work of breathing and improving breathing pattern in CF patients. Our objective was to compare the effects of HFNT versus NIV in terms of work of breathing, assessed noninvasively by the thickening fraction of the diaphragm (TFdi, measured with ultrasound), breathing pattern, transcutaneous CO2 (PtcCO2), hemodynamics, dyspnea and comfort.
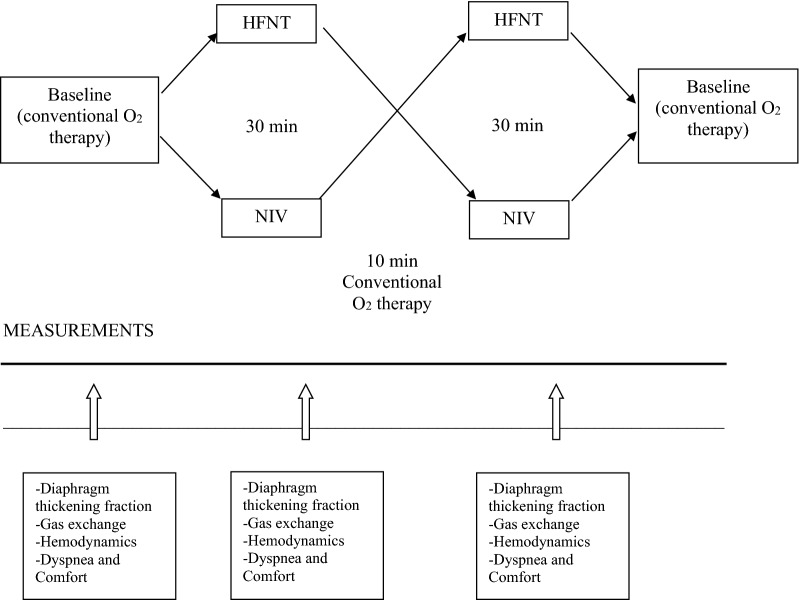
Methods: Adult CF patients who had been stabilized after requiring ventilatory support for a few days were enrolled and ventilated with HFNT and NIV for 30 min in crossover random order.
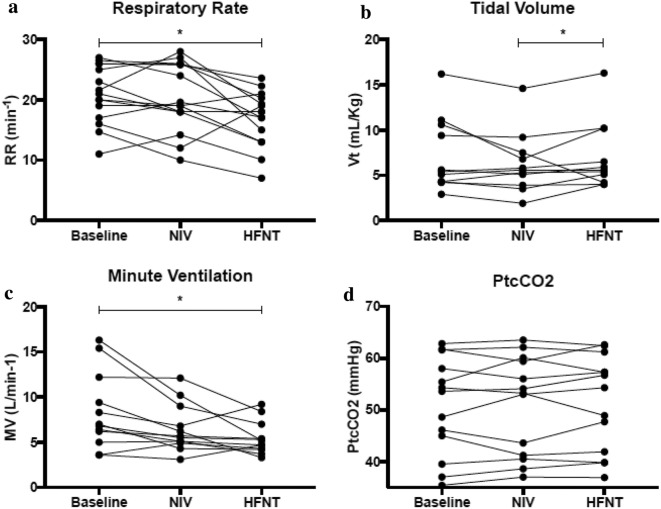
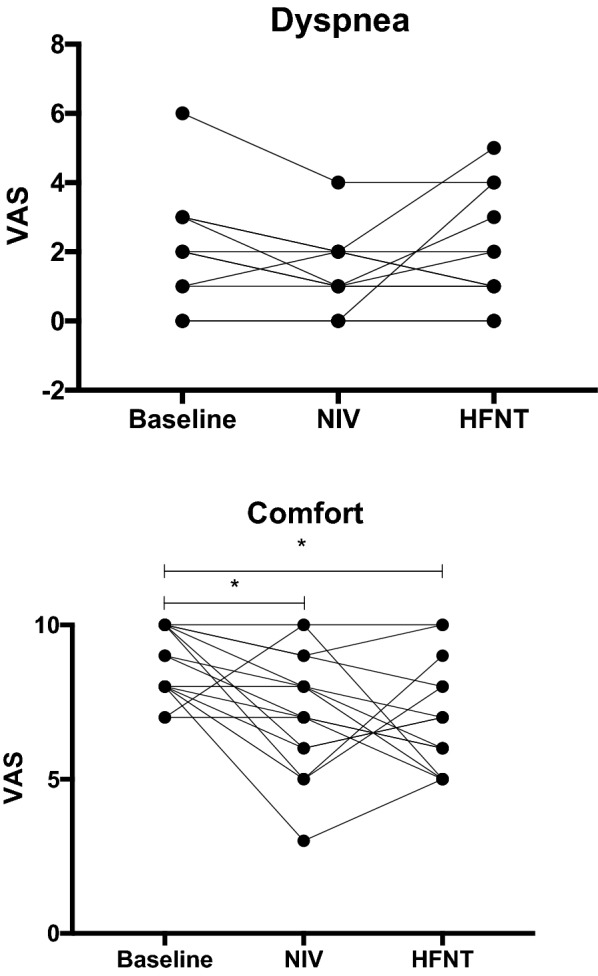
Results: Fifteen patients were enrolled. Compared to baseline, HFNT, but not NIV, reduced respiratory rate (by 3 breaths/min, p = 0.01) and minute ventilation (by 2 L/min, p = 0.01). Patients also took slightly larger tidal volumes with HFNT compared to NIV (p = 0.02). TFdi per breath was similar under the two techniques and did not change from baseline. MAP increased from baseline with NIV and compared to HFNT (p ≤ 0.01). Comfort was poorer with the application of both HFNT and NIV than baseline. No differences were found for heart rate, SpO2, PtcCO2 or dyspnea.
Conclusions: In adult CF patients stabilized after indication for ventilatory support, HFNT and NIV have similar effects on diaphragmatic work per breath, but high-flow therapy confers additional physiological benefits by decreasing respiratory rate and minute ventilation.
Clinical trial registration: Ethics Committee of St. Michael's Hospital (REB #14-338) and clinicaltrial.gov (NCT02262871).
Figures
Comment in
-
High-flow oxygen therapy for the management of patients with acute exacerbation of cystic fibrosis.Ann Transl Med. 2018 Dec;6(Suppl 2):S113. doi: 10.21037/atm.2018.11.67. Ann Transl Med. 2018. PMID: 30740434 Free PMC article. No abstract available.
-
High flow oxygen therapy and the work of breathing assessed by thickening fraction of the diaphragm (TFdi): just a side of the moon in cystic fibrosis patients?Ann Transl Med. 2019 Feb;7(3):58. doi: 10.21037/atm.2018.12.54. Ann Transl Med. 2019. PMID: 30906762 Free PMC article. No abstract available.
References
-
- Davies JC, Alton EWFW, Bush A. Cystic fibrosis. BMJ. 2007;335:1255–1259. doi: 10.1136/bmj.39391.713229.AD. - DOI - PMC - PubMed
-
- Fauroux B. Why, when and how to propose noninvasive ventilation in cystic fibrosis? Minerva Anestesiol. 2011;77:1108–1114. - PubMed
-
- Fauroux B, Burgel P-R, Boelle P-Y, Cracowski C, Murris-Espin M, Nove-Josserand R, et al. Practice of noninvasive ventilation for cystic fibrosis: a nationwide survey in France. Respir Care. 2008;53:1482–1489. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
