

Unexpected finding of uniparental disomy mosaicism in term placentas: Is it a common feature in trisomic placentas?
- PMID: 30187503
- PMCID: PMC6282787
- DOI: 10.1002/pd.5354
Unexpected finding of uniparental disomy mosaicism in term placentas: Is it a common feature in trisomic placentas?
Abstract
Objective: Non-invasive prenatal testing (NIPT) detects placental chromosome aberrations. When amniocentesis reveals a normal karyotype, confined placental mosaicism (CPM) may be assumed. In order to confirm this, placental cytogenetic studies were performed.
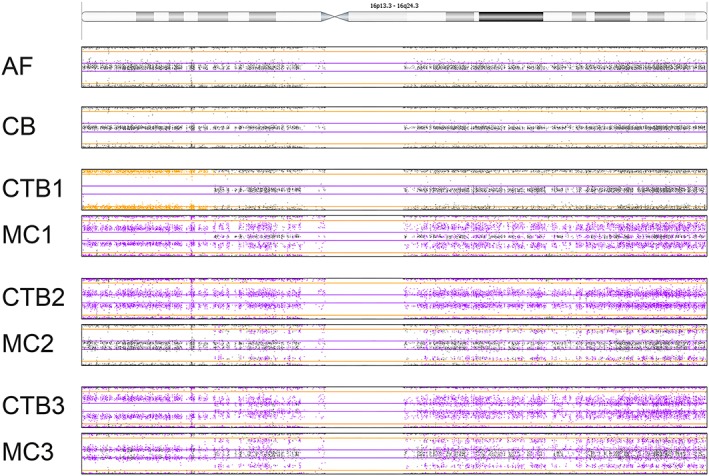
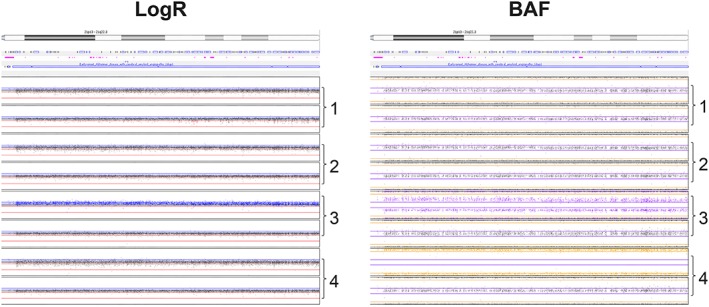
Method: NIPT was conducted in the course of the Dutch TRIDENT study. Placentas of 10 cases with NIPT results indicating an autosomal trisomy and showing a normal (N = 9) or low mosaic karyotype (N = 1) in amniotic fluid (AF) were investigated. The cytotrophoblast as well as the mesenchymal core of two to four placental chorionic villi biopsies were studied with single nucleotide polymorphism (SNP) array. Clinical outcome data were collected.
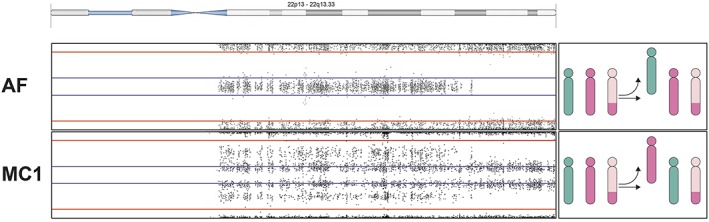
Results: In 10/10 cases, CPM was proven. In 3/10 cases trisomy/uniparental disomy (UPD)/biparental disomy (BPD) mosaicism was discovered. In 2/3 cases, all three cell lines were present in the placenta, whereas BPD was found in AF. In 1/3 cases trisomy 22/UPD22 was present in AF while trisomy 22/BPD22 mosaicism was found in the placenta. Five of 10 pregnancies were affected with pre-eclampsia, low birth weight, preterm delivery, and/or congenital malformations.
Conclusion: The presence of trisomy/UPD/BPD mosaicism in 3/10 cases that we investigated proves that trisomic zygote rescue may involve multiple rescue events during early embryogenesis. UPD mosaicism, when present in crucial fetal tissues, may explain the abnormal phenotype in undiagnosed cases.
© 2018 The Authors Prenatal Diagnosis Published by John Wiley & Sons Ltd.
Figures
Similar articles
-
Application of non-invasive prenatal testing in late gestation in a pregnancy associated with intrauterine growth restriction and trisomy 22 confined placental mosaicism.Taiwan J Obstet Gynecol. 2017 Oct;56(5):691-693. doi: 10.1016/j.tjog.2017.09.001. Taiwan J Obstet Gynecol. 2017. PMID: 29037560
-
Prenatal diagnosis of maternal uniparental disomy 5 by amniocentesis associated with confined placental mosaicism for trisomy 5 and fetal trisomy 21 in a pregnancy.Taiwan J Obstet Gynecol. 2020 Nov;59(6):938-940. doi: 10.1016/j.tjog.2020.09.023. Taiwan J Obstet Gynecol. 2020. PMID: 33218416
-
The maternal uniparental disomy of chromosome 6 (upd(6)mat) "phenotype": result of placental trisomy 6 mosaicism?Mol Genet Genomic Med. 2017 Nov;5(6):668-677. doi: 10.1002/mgg3.324. Epub 2017 Sep 22. Mol Genet Genomic Med. 2017. PMID: 29178649 Free PMC article.
-
[Study of a fetus with confined placental mosaicism for trisomy 2 in conjunct with fetal uniparental disomy and a literature review].Zhonghua Yi Xue Yi Chuan Xue Za Zhi. 2023 Dec 10;40(12):1461-1465. doi: 10.3760/cma.j.cn511374-20220524-00348. Zhonghua Yi Xue Yi Chuan Xue Za Zhi. 2023. PMID: 37994124 Review. Chinese.
-
Maternal uniparental disomy 16 and genetic counseling: new case and survey of published cases.Genet Couns. 2004;15(2):183-90. Genet Couns. 2004. PMID: 15287418 Review.
Cited by
-
Detecting mitochondrial mutations associated with aminoglycoside ototoxicity by noninvasive prenatal testing.J Clin Lab Anal. 2023 Jan;37(1):e24827. doi: 10.1002/jcla.24827. Epub 2022 Dec 29. J Clin Lab Anal. 2023. PMID: 36579624 Free PMC article.
-
Clinical Selection of Prenatal Diagnostic Techniques Following Positive Noninvasive Prenatal Screening Results in Southwest China.Front Genet. 2022 Jan 28;12:811414. doi: 10.3389/fgene.2021.811414. eCollection 2021. Front Genet. 2022. PMID: 35154255 Free PMC article.
-
Prenatal Detection of Uniparental Disomies (UPD): Intended and Incidental Finding in the Era of Next Generation Genomics.Genes (Basel). 2020 Dec 3;11(12):1454. doi: 10.3390/genes11121454. Genes (Basel). 2020. PMID: 33287348 Free PMC article. Review.
-
Placental studies elucidate discrepancies between NIPT showing a structural chromosome aberration and a differently abnormal fetal karyotype.Prenat Diagn. 2019 Oct;39(11):1016-1025. doi: 10.1002/pd.5531. Epub 2019 Aug 13. Prenat Diagn. 2019. PMID: 31321790 Free PMC article.
-
Preimplantation chromosomal mosaics, chimaeras and confined placental mosaicism.Reprod Fertil. 2022 Apr 5;3(2):R66-R90. doi: 10.1530/RAF-21-0095. eCollection 2022 Apr 1. Reprod Fertil. 2022. PMID: 35514539 Free PMC article. Review.
References
-
- Hahnemann JM, Vejerslev LO. European collaborative research on mosaicism in CVS (EUCROMIC)—fetal and extrafetal cell lineages in 192 gestations with CVS mosaicism involving single autosomal trisomy. Am J Med Genet. 1997;70(2):179‐187. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
