

What Factors Are Associated With Disability After Upper Extremity Injuries? A Systematic Review
- PMID: 30188344
- PMCID: PMC6259989
- DOI: 10.1097/CORR.0000000000000427
What Factors Are Associated With Disability After Upper Extremity Injuries? A Systematic Review
Erratum in
-
Erratum to: What Factors Are Associated With Disability After Upper Extremity Injuries? A Systematic Review.Clin Orthop Relat Res. 2019 May;477(5):1256. doi: 10.1097/CORR.0000000000000730. Clin Orthop Relat Res. 2019. PMID: 30998644 Free PMC article. No abstract available.
Abstract
Background: Psychosocial factors are key determinants of health after upper extremity injuries. However, a systematic review is needed to understand which psychosocial factors are most consistently associated with disability and how the language, conceptualization, and types of measures used to assess disability impact these associations in upper extremity injuries.
Questions/purposes: (1) What factors are most consistently associated with disability after upper extremity injuries in adults? (2) What are the trends in types of outcome measures and conceptualization of disability in patients' upper extremity injuries?
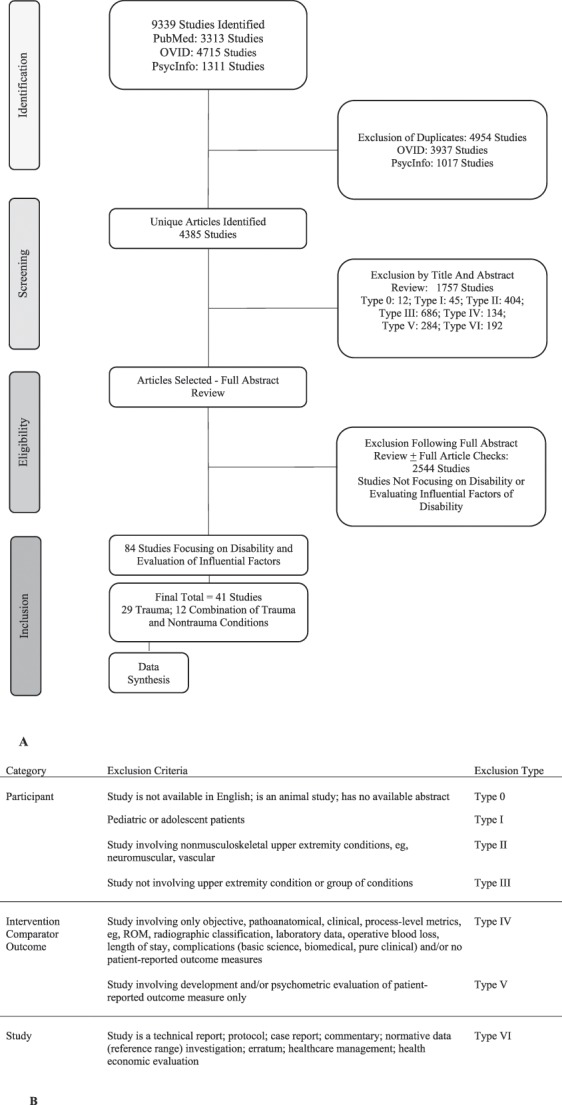
Methods: We searched multiple electronic databases (PubMED, OVIDSP, PsycInfo, Google Scholar, ISI Web of Science) between January 1, 1996, and December 31, 2016, using terms related to the "upper extremity", "outcome measurement", and "impairment, psychological, social or symptomatic" variables. We included all studies involving adult patients with any musculoskeletal injury and excluded those that did not use patient-reported outcome measures. We identified and screened 9339 studies. Of these, we retained 41 studies that involved conditions ranging from fractures to soft tissue injuries in various regions of the arm. We conducted quality assessment using a 10-item validated checklist and a five-tier strength of evidence assessment. We used the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) criteria and registered the review before performing our search (PROSPERO: CRD42017054048). None of the authors received any funding to perform this work.
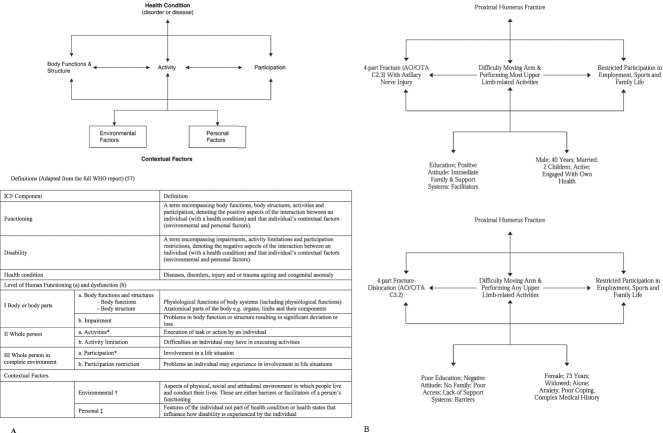
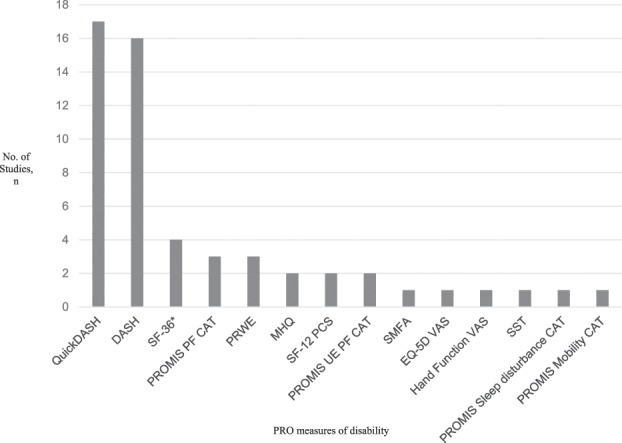
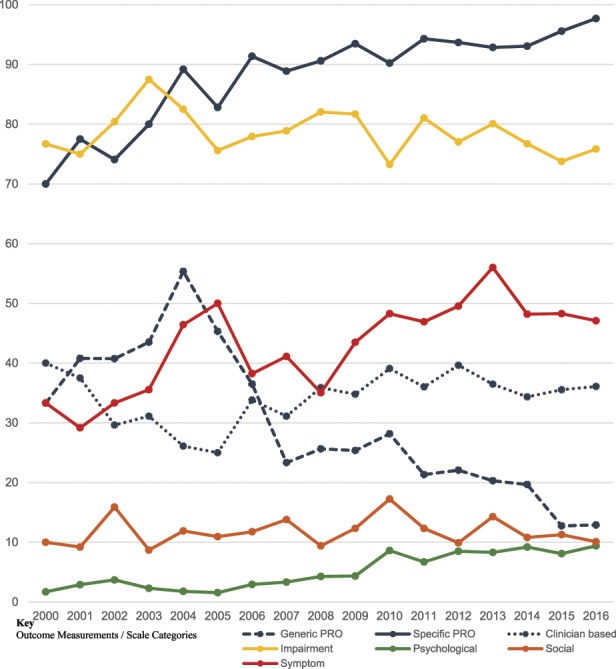
Results: Disability after upper extremity injury was most consistently associated with depression (21 cohorts), catastrophic thinking (13 cohorts), anxiety (11 cohorts), pain self-efficacy (eight cohorts), and pain interference (seven cohorts). Social and demographic factors were also associated with disability. Measures of impairment such as ROM and injury severity were least associated with disability. There has been a gradual increase in use of region or condition-specific patient-reported outcome measures and measures of psychological, social, and symptomatic factors over a period since the introduction of the World Health Organization (WHO) International Classification of Functioning, Disability and Health (ICF) around 2000. Approximately 17% of studies (n = 454 of 2628) had instances of unclear, conflicting, or inappropriate terminology and 11% of studies (n = 257 of 2628) involved misrepresentations of outcome measures related to disability.
Conclusions: Psychologic and social factors are most consistently associated with disability than factors related to impairment. Further research involving the assessment of depression, anxiety, and coping strategies in cohorts with specific injuries may support decision-making regarding the provision of emotional support and psychologic therapies during recovery. Using the WHO ICF framework to conceptualize disability is key in increasing strength of evidence and allowing accurate comparisons of research in this field.
Level of evidence: Level IV, therapeutic study.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: What Factors Are Associated With Disability After Upper Extremity Injuries? A Systematic Review.Clin Orthop Relat Res. 2018 Nov;476(11):2216-2218. doi: 10.1097/CORR.0000000000000498. Clin Orthop Relat Res. 2018. PMID: 30247230 Free PMC article. No abstract available.
References
-
- Ariens GAM, van Mechelen Q, Bongers PM, Bouter LM. Physical risk factors for neck pain. Scand J Work Environ Health. 2000;26:7–19. - PubMed
-
- Bear-Lehman J, Poole SE. The presence and impact of stress reactions on disability among patients with arm injury. J Hand Ther. 2011;24:89–94. - PubMed
-
- Bekkers S, Becker SJE, Bossen JKJ, Mudgal CS, Ring D, Vranceanu AM. Relationships between pain misconceptions, disability, patient’s goals and interpretation of information from hand therapists. J Hand Ther. 2014;27:287–295. - PubMed
-
- Bot A, Bekkers S, Herndon J, Mudgal CS, Jupiter JB, Ring D. Determinants of disability after proximal interphalangeal joint sprain or dislocation. Psychosomatics. 2014;55:595–601. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
